11/08/2025
Professor Bhavani Rao
URETHRALSTRICTURES
INTRODUCTION
• Fibrotic narrowing of urethra due to
scarring.
• Causes obstructive urinary symptoms
and complications.
• Common in males, especially post
instrumentation or trauma.
11/08/2025
Professor Bhavani Rao
DEFINITIVEMANAGEMENT
• Dilatation - Temporary relief, high recurrence.
• VIU - For short strictures, recurrence
common.
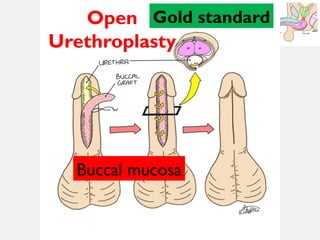
• Open Urethroplasty - Gold standard for long
strictures.
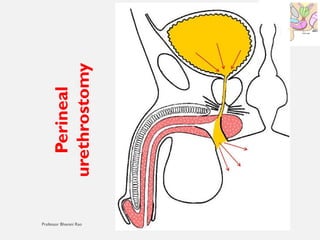
• Perineal urethrostomy - For
complex/recurrent cases.
#1 For MBBS Students - As per NMC Curriculum
Address through web cam
https://onedrive.live.com/personal/410986d2df077281/_layouts/15/Doc.aspx?resid=410986D2DF077281!seadc29dcb78c420eac9f603b94ad7f4a&cid=410986D2DF077281&migratedtospo=true&app=PowerPoint
Deep dive
QR code
Song
#2 “Imagine a 35-year-old man walks into your OPD with complaints of poor urinary stream and straining to pass urine for the past few months…”
Urethral stricture is a fibrotic narrowing of the urethra due to scarring of the urethral epithelium and underlying spongy tissue (corpus spongiosum).
• It leads to obstruction of urinary flow, recurrent infections, and sometimes upper tract damage.
A hallmark clinical feature of urethral stricture is:
Poor urinary flow
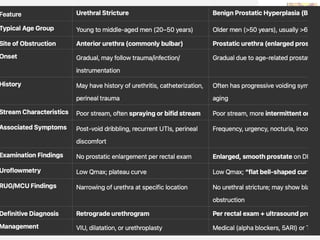
#3 A young man with obstructive symptoms and a history of catheterization is more likely to have urethral stricture, whereas an elderly gentleman with poor stream and nocturia is more likely to have BPH.”
“Young man → Think Stricture; Old man → Think Prostate.”
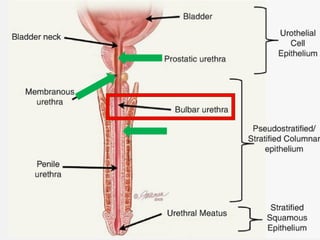
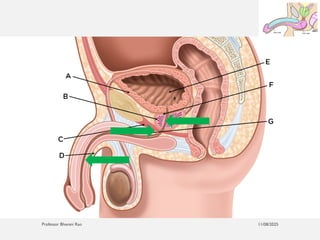
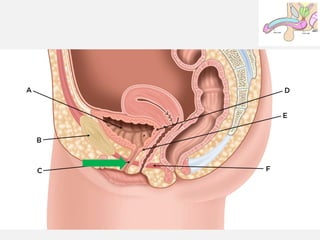
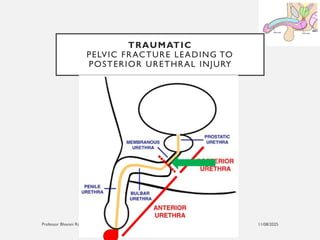
#4 Male urethra Anatomy anterior view
Bulbar part of urethra most commonly involved in strictures
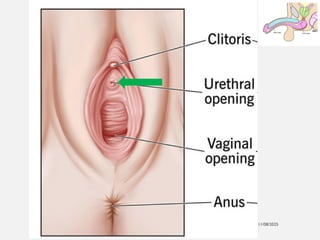
#7 How to Find the Female Urethral Opening (External Urethral Meatus)
1. Anatomical Location
• The female external urethral opening is:
• Situated in the vestibule of the vulva.
• Lies just above the vaginal opening (introitus).
• Located below the clitoris, approximately 2.5 cm below the clitoral glans.
• Appears as a small slit or round opening.
#16 Irritative:
• Frequency
• Urgency
• Dysuria
🔶 Other Clinical Clues:
• Recurrent UTIs
• Perineal discomfort
• Spraying of urine
• Urinary tract stones or secondary hydroureteronephrosis
• Acute urinary retention if complete blockage
#17 Remember the “obstructive and irritative symptoms”.
A 40-year-old male has recurrent UTI and post-void dribbling. Likely diagnosis:
poor stream is not a typical irritative symptom
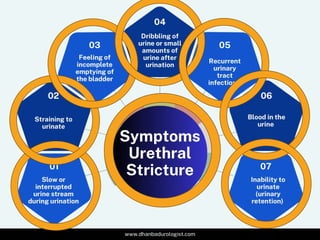
🔶 Lower Urinary Tract Symptoms (LUTS):
• Obstructive:
• Poor urinary stream
• Straining to void
• Intermittent stream
• Post-void dribbling
• Incomplete emptying
• Urinary retention (in severe cases)
• Irritative:
• Frequency
• Urgency
• Dysuria
🔶 Other Clinical Clues:
• Recurrent UTIs
• Perineal discomfort
• Spraying of urine
• Urinary tract stones or secondary hydroureteronephrosis
• Acute urinary retention if complete blockage
#18 Examination
🔸 General:
• Look for signs of infection, fever, dehydration.
🔸 Local (Genital and Perineal Exam):
• Palpate for:
• Periurethral induration
• Perineal scarring or fistula
• Bladder distension on abdominal exam.
🔸 Digital Rectal Examination:
• To rule out associated prostatitis or prostatic pathology.
#19 Investigations
Divide this into:
✅ Basic Investigations:
• Urine Routine & Culture – to rule out infection.
• Blood Urea, Serum Creatinine – to assess renal function.
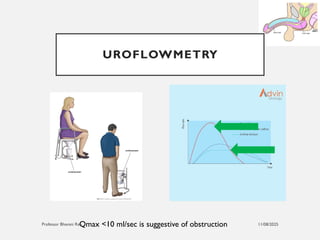
#20 Measures peak flow rate (Qmax <10 ml/sec is suggestive of obstruction).
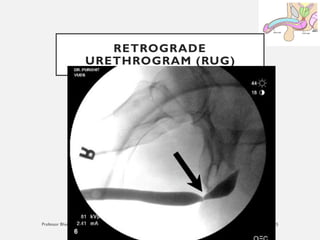
#21 Retrograde Urethrogram (RUG):
• Gold standard.
• Helps localize and measure the length of the stricture.
• Especially useful in anterior urethral strictures.
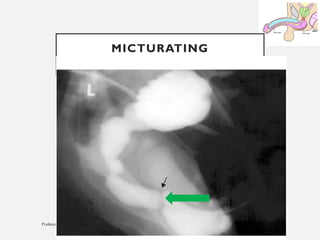
#22 Micturating Cystourethrogram (MCU):
• Useful to study posterior urethra and bladder neck.
• Shows stricture with proximal urethral dilatation.
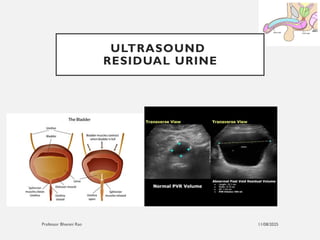
#23 Ultrasound KUB + Post-void Residual Urine:
• Detects residual urine, bladder wall thickening, hydronephrosis.
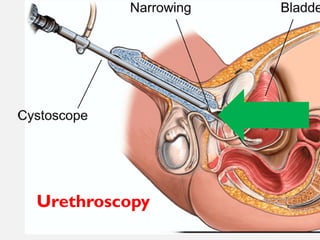
Urethroscopy (Endoscopy):
• Direct visualization of the stricture.
• Useful in therapeutic planning.
#26 Acute Management:
• If in urinary retention:
• Suprapubic catheterization may be required if urethral catheterization fails.
Treat infections with antibiotics.
#27 Definitive Treatment Options:
1. Dilatation:
• Gradual dilatation using filiforms and followers or metal sounds.
• High recurrence rate.
• Done as an initial/temporary measure or in poor surgical candidates.
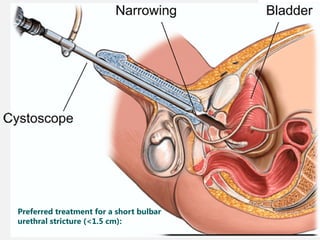
#28 Preferred treatment for a short bulbar urethral stricture (<1.5 cm):
Visual Internal Urethrotomy (VIU):
• Done under endoscopic guidance.
• Suitable for short strictures <1.5 cm.
• High recurrence if long segment or multiple strictures.
• Recurrence rate ~30–70%.
#29 Open Urethroplasty:
• Gold standard for long/recurrent strictures.
• Types:
• End-to-End anastomotic urethroplasty (for short bulbar strictures).
• Substitution urethroplasty using grafts (buccal mucosa) or flaps.
• Low recurrence rates.
• Technically demanding.
#30 Perineal urethrostomy:
• Used in complex or failed cases, often elderly patients.
#34
Birds Upper Open urethral strictures, word document
Lower deep dive
Command (⌘) + F1. or Command (⌘) + Fn + F1
https://notebooklm.google.com/notebook/2206370b-3e60-4bd6-9a97-330e7e9b2d8d/audio
#36 “The Stricture Song (Urethra Highway Blues)” 🎸
(To the tune of a classic toe-tappin’ country song)
[Verse 1]
Well, I woke up feelin’ funny, couldn’t pee like I used to do,
That stream was weak, it sprayed a bit—felt like a leaky ol’ canoe.
Went down to see my doctor, he gave me quite the news,
Said “Son, it’s a stricture on your urethral route—ain’t that a funky fuse?”