Downloaded 20 times
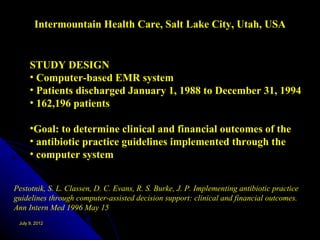
![1982-1984 Non clinical evaluation
1984-1986 physician involvement and evaluation
1984-1987 ABSTRACT[SUMMARISATION] modification and implementation (Continuing evolution)
1986-1987 Modification of program / dictionaries /screen displays / reports / units of measurement
1986 MANUAL data entry of laboratory data
1987 MANUAL data entry by NURSING STAFF of clinical / protocol / chemotherapy data
1988-1989 AUTOMATED LABORATORY DATA TRANSFER
1989 REPORT GENERATOR functions(FLOWS &PLOTS)
• DRG diagnostic data electronically collated for administration [2nd art to
CLINICAL DATA].
CLINICAL TRAILS module implemented
1990-1992 Protocol generated care plans tested and evaluated
10 years
Hannan, T., International transfer of the Johns Hopkins Oncology Center clinical information
system. MD Comput, 1994. 11(2): p. 92-9.](https://image.slidesharecdn.com/unsw28june2012final-120708195016-phpapp02/85/UNSW-from-OCIS-to-OpenMRS-3-320.jpg)

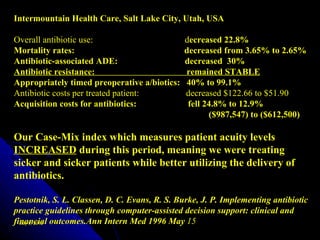
![TECHNOLOGY IS NOT THE PROBLEM
[30 years EMR experience and research]
Retrieval times-Fast (blink times)
Data and information-Comprehensive
Data storage- Long-term-lifelong
Data applications-Introspective of total database
Data storage-
200 million coded observations By products of the care process
3.25 million narrative reports RESEARCH-accuracy / $
15 million prescriptions EPIDEMIOLOGY
212,000 ECG tracings ADMIN SUPPORT
More than 1.3 million patients “Record once use many times”
Access-
1300 medical nurses
1000 physicians
220 medical students
Across health care institutions (16)
Data access more than 628,000 / month
C.J. McDonald, et al, The Regenstrief Medical Record System: A quarter century experience. Int J
July 9, 2012Inform 54 (1999), 225‑ 253.)
Med](https://image.slidesharecdn.com/unsw28june2012final-120708195016-phpapp02/85/UNSW-from-OCIS-to-OpenMRS-8-320.jpg)
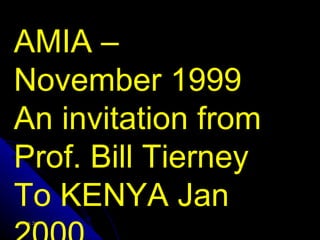
![CCDSS TOOLS IN CLINICAL MEDICINE-REQUIREMENTS
1.ALERTING
2. REMINDING
3. INTERPRETATION
4.ASSISTING
5.CRITIQUING
6.DIAGNOSING
7.MANAGING
8. KNOWLEDGE ACCESS /COUPLING
[“Medicine in Denial.” L.Weed,L.Weed.2011]
Pryor TA, Clayton PD. Decision support systems for clinical medicine.
July 9, 2012 9
Tutorial 11.15th SCAMC.Nov. 17. 1991.](https://image.slidesharecdn.com/unsw28june2012final-120708195016-phpapp02/85/UNSW-from-OCIS-to-OpenMRS-9-320.jpg)
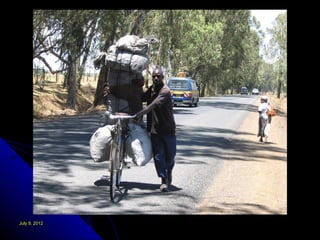








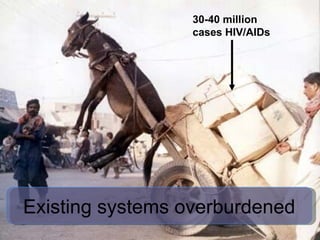
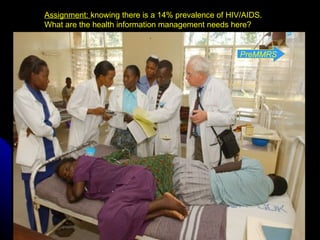
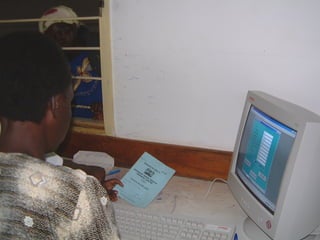


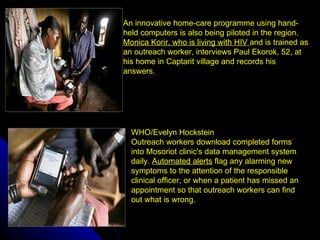
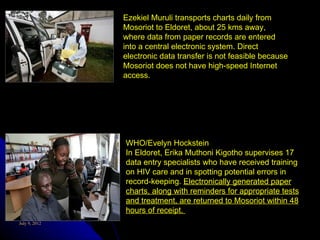


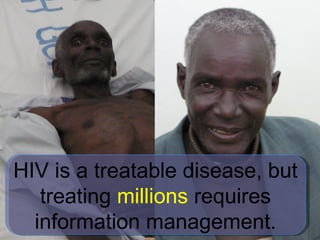
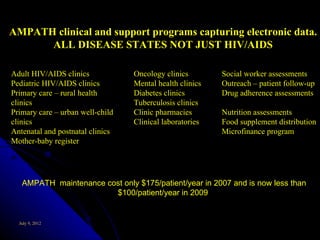



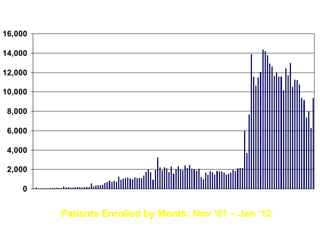
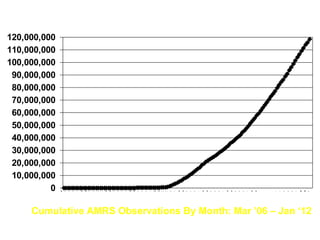

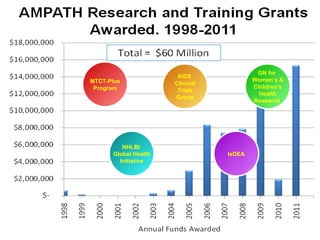
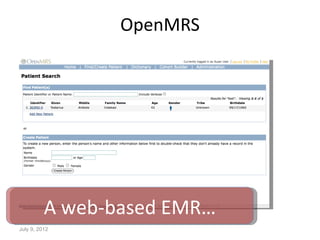
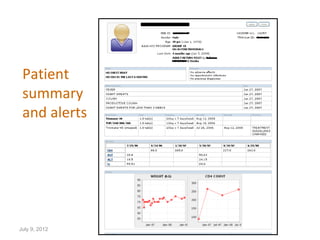
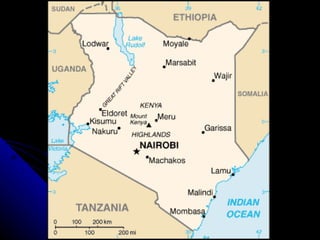




The document discusses the implementation and success of e-health systems in resource-poor economies, particularly in Kenya, highlighting the evolution of clinical information systems and their impact on healthcare management. It emphasizes the significance of data management in improving patient care, especially in the context of HIV/AIDS, and showcases collaborative efforts in establishing health information systems. Additionally, it outlines the benefits of electronic medical records in enhancing clinical outcomes and resource utilization.



































































