
Recommended
More Related Content
Similar to Unit 4 Review Assignment Please write in complete sentences. You.docx
Similar to Unit 4 Review Assignment Please write in complete sentences. You.docx (20)
More from marilucorr
More from marilucorr (20)
Recently uploaded
Recently uploaded (20)
Unit 4 Review Assignment Please write in complete sentences. You.docx
- 1. Unit 4 Review Assignment Please write in complete sentences. You should work on this assignment as you go through the assigned readings and chapters in your textbook. Avoid copying directly from the text. Your responses should be in your own words. Chapter 8 1. Explain how listening helps to earn trust, to build collaboration and to negotiate resolutions to problems and conflicts. 1. Imagine you manage 100 employees. Some employees work in the home office, and others remotely in other cities. Identify and describe two ways you might encourage communication among these 100 people. 2. Describe two specific actions a leader might take to develop cooperative goals. 3. What is reciprocity? Why is reciprocity a successful approach for making daily decisions and negotiating differences among people? Chapter 9 6. Explain the relationship between leadership and control. 7. Explain what is meant by the phrase “in the flow.” 8. Identify and explain two methods or ways to increase skill and competency. 9. Explain the difference between training and coaching.
- 2. Identify one way or technique you might use to coach a new employee. The Leadership Challenge Workbook 10. Your textbook focuses on the importance of building trust and recommends holding a one-on-one relationship building meeting to foster trust. On page 97 of your Workbook, you will see a list of questions that you might ask during such a meeting. Select three of these questions from the list and explain why you would consider these three the most important. Introduction Research relating to the effects of exercise on glycaemic control in people with type 1 diabetes has usu- ally been performed in laboratory environments.1–5 A recent literature review was performed to identify any related research where the replica- tion of laboratory based self-manage- ment research findings were applied into the real-life environment, and also to demonstrate any differences regarding the impact on glycaemic control between environments. It became evident that all research identified regarding self-manage- ment was based in a laboratory envi- ronment using either a treadmill or bicycle for exercise, and not applied into real-life situations.2–5 However, the knowledge generated from these
- 3. laboratory based experiments under- pins current self-management rec- ommendations.2–4,6–11 From these original studies and literature review publications, a self-management algorithm for use when performing moderate intensity exercise before the evening meal was devised (see Table 1). The aim of this current study was to compare the glucose response in participants with type 1 diabetes, during and after a 40-minute exer- cise session at 70% VO2 max (mod- erate intensity exercise) while following the self-management algo- rithm, in the laboratory environ- ment using a treadmill, and while running in participants’ real-life environment. This was to evaluate the efficacy of using laboratory find- ings, under controlled conditions, in patient education for use in their everyday life. The significance and value of real-world data are becom- ing an increasingly valuable source of evidence for clinical practice.12 PRACTICAL DIABETES VOL. 32 NO. 6 COPYRIGHT © 2015 JOHN WILEY & SONS 217 Original article Can laboratory based research regarding
- 4. type 1 diabetes and exercise be applied into the real-life environment? Abstract The aim of this study was to determine whether results from laboratory based research examining glycaemic control during and after exercise can be applied to a real-life (non-laboratory) environment. A comparative study of individuals with type 1 diabetes (n=9) using basal bolus analogue insulin regimens was undertaken. Glycaemic control before and after two 40-minute runs at 70% VO2 max, in both laboratory and real-life environments, was measured across 10 time-points during and up to 12 hours after exercise. Insulin was adjusted in all participants following a self-management algorithm. Pooled mean glucose concentrations at each time-point were compared. There was no statistically significant difference (F[1, 8] = 1.489, p=0.257) in overall mean glucose concentrations between environments. Similarly, the exercise environment or time-point of measurement had no statistically significant effect on mean glucose concentration (F[9, 72] = 0.499, p=0.871). However, during exercise, episodes of both hypoglycaemia (<4.0mmol/L) and hyperglycaemia (>9.0mmol/L) were more frequent in the laboratory environment than in the real-life environment: 5 vs 1 and 25 vs 19 episodes, respectively; the frequency of acceptable concentrations (4.0–9.0mmol/L) was greater in the real-life environment (24 vs 34). In the 8–12
- 5. hours after exercise, hypoglycaemia occurred more frequently in the real-life environment (3 vs 8) with hyperglycaemia occurring more frequently in the laboratory environment (22 vs 14); again, there were slightly increased acceptable concentrations in the real-life environment (29 vs 33). The exercise environment does not appear to affect overall mean blood glucose concentrations. However, it may affect the timing and frequency of hypoglycaemia and hyperglycaemia. Copyright © 2015 John Wiley & Sons. Practical Diabetes 2015; 32(6): 217–221 Key words type 1 diabetes; moderate intensity exercise; laboratory and real-life environments; glycaemic control Jacqui Charlton MRes, BSc, PgCTLHE, RGN, Lecturer and Specialist Nurse in Diabetes, Metabolic Unit, Western General Hospital, Edinburgh; Edinburgh Napier University, UK Lynn Kilbride PhD, MSc, BA (Hons), PGCE, Head of School, Glasgow Caledonian University, Glasgow, UK Rory MacLean PhD, MBPsS, FHEA, BSc (Hons), Lecturer in Psychology, Sighthill Campus, Edinburgh Napier University, Edinburgh, UK Mark G Darlison FSB, PhD, MSc, BSc, Professor of Neuroscience, and
- 6. Director of Research for the Faculty of Health, Life and Social Sciences, Sighthill Campus, Edinburgh Napier University, Edinburgh, UK John McKnight MB, BCh, MRCP, MD, FRCP, Consultant Physician, Metabolic Unit, Western General Hospital, Edinburgh, UK Correspondence to: Miss Jacqui Charlton, Room 4B16, Sighthill Campus, Edinburgh Napier University, Edinburgh EH11 4BN, UK; email: [email protected] Received: 13 January 2015 Accepted in revised form: 6 March 2015 This supports the question of whether data collected in a con- trolled and possibly unrealistic laboratory environment would be replicated when performed in a real- life environment. Method The inclusion criteria for partici- pants were: people with type 1 dia- betes of over two years’ duration; aged 18–60 years old; HbA1c under 86mmol/mol (10.0%); using a basal bolus insulin regimen; hypogly- caemia awareness; and exercise twice a week or more. The exclusion criteria were: pre-
- 7. proliferative/proliferative retinopa- thy; neuropathy/foot ulceration; blood pressure >150/90; cardiovas- cular disease/history of angina; orthopaedic problems. Study design The study ran over a two-week period. On days 1 and 3 of each week, participants undertook 40 minutes of moderate intensity exer- cise (days 1 and 8 in the laboratory, and days 3 and 10 in real-life environments). Days 2 and 9 were rest days and participants were instructed not to perform exercise. All were instructed to follow the self-management algorithm for insulin and carbohydrate adjust- ment (Table 1). Data collection The data collection methods for glucose levels were: • Before exercise until before evening meal: participants per- formed self-monitoring of blood glu- cose (SMBG) using a TrueResult meter (Nipro Diagnostics UK). This meter was chosen due to ease of use and small size for carrying in the exercise sessions. SMBG was chosen for this time-period as it was impor- tant to establish any immediate changes in blood glucose that may require cessation of exercise.
- 8. • After the evening meal until 12 hours after: interstitial glucose levels using the Minimed iPro (Medtronic) continuous glucose meter were used. This method was used as this time-period was during the night and performing SMBG would disturb participants’ sleep. The continuous glucose monitoring 218 PRACTICAL DIABETES VOL. 32 NO. 6 COPYRIGHT © 2015 JOHN WILEY & SONS Can laboratory based research regarding type 1 diabetes and exercise be applied into the real-life environment? Original article Lunchtime insulin • If exercising within 2 hours of eating a meal, reduce the bolus/meal dose by 75%3,4 Blood glucose • Aim for blood glucose of 8mmol/L immediately before exercise • If blood glucose over 12mmol/L, check for ketones and take a correction dose • If blood glucose over 17mmol/L do not exercise8–11 Food • If blood glucose under 8mmol/L have the following carbohydrate (CHO)1,14 Blood glucose prior to exercise (mmol/L) Amount of CHO (g) Under 4 30
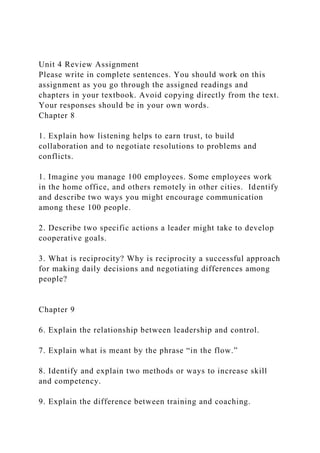
- 9. 4–6 20 6–8 10 8 or over 0 Bolus/meal insulin • Eat within 2 hours of exercise and reduce the bolus/meal dose by 30%3,9–11 • After 2 hours return to usual dose Long-acting insulin • Take usual Lantus or Levemir dose2 Blood glucose • If blood glucose at 8mmol/L or under before bedtime have 10– 20g of CHO Table 1. Algorithm for insulin and carbohydrate adjustment for exercising at 70% VO2 max Before exercise After exercise Figure 1. A comparison of mean blood glucose concentrations in laboratory and real-life sessions. The error bars represent standard deviations Bl oo d gl
- 12. l 2 h ou rs aft er 6 h ou rs aft er 8 h ou rs aft er 10 ho urs af ter 12 ho urs af ter
- 13. data were only available by download after the study period. In order to ensure reliability of the comparison of environments, it was important that the exercise sessions were consistent, i.e. performed at the same time of day, following the same self-management algorithm, and exercising at the same intensity. In the laboratory sessions, the treadmill was used which was considered best to replicate running in a real-life environment. The intensity was con- trolled by manipulating the speed and grade to ensure that 70% VO2 max was achieved, which equates to moderate intensity exercise.13 This was pre-determined by a sub-maxi- mal incremental walking test to determine an individual’s 70% VO2 max. In the real-life sessions, partici- pants undertook running outside or in a sports hall in an area of their choice. Participants were given an individual training heart rate (THR) with a minimum and maximum range, which again was determined by the sub-maximal incremental walking test. They used a Polar wrist- watch during the exercise sessions to ensure their HR was within the target range and this ensured the mainte- nance of 70% VO2 max. Analysis
- 14. Statistical. The four exercise sessions were analysed using the mean blood glucose concentrations and standard deviations using a three-way repeated measures test (ANOVA) to explore any differences in blood glucose measured in mmol/L between the two environments (laboratory or real- life), and in the two sessions (i.e. week one and week two), across 10 time-points: before exercise, 20 min- utes during, at 40 minutes [end of session], before the evening meal, and at 2, 4, 6, 8, 10 and 12 hours after. Bonferroni adjustments were used to control the probability of finding type 1 errors. Statistical significance was set at p<0.05. Data are presented as means ± standard deviation. Descriptive. A descriptive analysis was also performed as the characteristics of the statistical tests along with the small participant numbers used would not reveal any extreme glucose episode outliers. Across the four exercise sessions all data were analysed for the occurrence of participant glycaemic episodes in dif- ferent glucose ranges: hypoglycaemia (≤4.0mmol/L); acceptable range (4–9mmol/L); and hyperglycaemia (≥9.0mmol/L). The frequencies of individual participant episodes for each of these ranges were stated as
- 15. numbers. There were 18 individual participant episodes (nine partici- pants: two sessions [laboratory or real- life]) for each time-point. This would demonstrate differences between time-points within environments. Results Nine individuals with type 1 diabetes (five male, four female) completed the study and performed four exer- cise sessions (two laboratory and two real-life). All used a basal bolus analogue insulin regimen and exer- cised regularly. The demographic data are presented as means ± standard deviation: age 39.3±10.5 years (range 24–56 years); BMI 24.8±1.7kg/m2; weight 75.6±6.2kg; HbA1c 63mmol/mol (7.9±0.7%); duration of diabetes 16.8±14.2 years (range 4–46 years). Mean glucose concentrations The pooled data of mean glucose concentrations taken at the specific time-point with standard deviations in the laboratory and real-life ses- sions are shown in Figure 1, which displays the comparison between environments. The mean glucose concentrations revealed similar results in both environments. However, the glucose concentrations appeared to be more variable at the
- 16. real-life time-points, which were recognised by the larger standard deviations, compared with the labo- ratory time-points. Differences between environments With the overall mean glucose con- centrations, the three-way ANOVA verified that the environment did not have a significant main effect on the glycaemic control of partici- pants (F[1, 8] = 1.489, p=0.257). This referred to the comparison of all mean glucose concentrations for both environments, without examining change in blood glucose over time. When investigating two-way inter- actions regarding glucose control between the variables, there were no significant effects on environments and times (F[9, 72] = 0.499, p=0.871). PRACTICAL DIABETES VOL. 32 NO. 6 COPYRIGHT © 2015 JOHN WILEY & SONS 219 Can laboratory based research regarding type 1 diabetes and exercise be applied into the real-life environment? Original article Table 2. A summary of episode percentages and numbers in time periods for each glucose range
- 17. Environment Lab Real-life Lab Real-life Lab Real-life Lab Real-life Blood glucose 9.3% 1.9% 5.6% 0 9.3% 3.7% 5.6% 14.8% under 4mmol/L (5) (1) (1) (0) (5*) (2*) (3) (8*) Blood glucose 44.4% 63% 55.6% 50% 46.3% 46.3% 53.7% 61.1% 4–9mmol/L (24) (34) (10) (9) (25) (25) (29) (33) Blood glucose 46.3% 35.2% 38.9% 50% 48.1% 51.9% 40.7% 25.9% over 9mmol/L (25) (19) (7) (9) (26) (28) (22) (14) *Additional hypoglycaemic episodes occurred in between the 2- hourly time-points. In the 2–6 hours after period, 2 of these occurred in the laboratory environment and 1 during the real-life environment. In the 8–12 hours after period, 1 occurred in the real-life environment. These occurrences have been included in the episode numbers. Baseline – 40 minutes Before evening meal 2–6 hours after 8– 12 hours after Descriptive analysis The episode percentage and num- bers for each glucose range at the different time periods are shown in Table 2. During exercise. When comparing the laboratory vs real-life environ- ment, episodes of both hypogly-
- 18. caemia (5 vs 1) and hyperglycaemia (25 vs 19) during exercise in the laboratory environment were more frequent than during real-life exer- cise, with greater acceptable concen- trations in the real-life environment (24 vs 34). Up to 6 hours after exercise. During the before evening meal time-point and up until 6 hours after exercise, increased hypoglycaemia occurred in the laboratory environment (6 vs 2). Similar episode frequencies were demonstrated in acceptable concen- trations (35 vs 34), and hypergly- caemia (33 vs 37). 8–12 hours after exercise. In the 8–12 hour time-period after exer- cise, when comparing the laboratory vs real-life environment, hypogly- caemia occurred more frequently in the real-life environment (3 vs 8) with hyperglycaemia occurring more frequently in the laboratory environment (22 vs 14); again, there were a slightly greater number of acceptable concentrations in the real-life environment (29 vs 33). Discussion The exercise session environments were designed to mimic each other, and the self-management algorithm used was the same for
- 19. both environments. One might pre- dict, therefore, that there would be no difference between the glucose responses in each environment. Statistically, no difference was found, but these findings were based on only nine participants and our study was therefore underpow- ered to detect a difference, as 12 participants were required for an 80% chance of detecting a 0.5% difference in glucose response. The three-way ANOVA showed no differences in glycaemic control between the laboratory and real- life environments. However, when the descriptive analysis (which highlighted extreme outliers) was performed using episodes of gly- caemic ranges – i.e. hypoglycaemia, acceptable range of 4–9mmol/L, and hyperglycaemia – important differences in glucose concentra- tions were apparent. Hypoglycaemia episodes. At 20 min- utes during exercise and at 40 min- utes (end of exercise session) there were higher hypoglycaemia episode numbers in the laboratory environ- ment. Whereas during the 8–12 hour period after the evening meal and fast-acting analogue insulin injection, there was an increase in
- 20. hypoglycaemia episodes in the real- life environment. Acceptable glucose range. Overall, the patterns suggested that the real-life sessions achieved greater 4–9mmol/L episodes compared with the laboratory sessions, except before the evening meal and 2 hours after the exercise time-points. For the whole of the experimental period from baseline to 12 hours post-exercise, the real-life environ- ment showed more episodes within the normal range (laboratory 88 vs real-life 101). However, it must be acknowledged that the mean glu- cose results in the real-life environ- ment did show higher standard deviations which suggest greater variability of glucose control. Hyperglycaemic episodes. It is appreciated that often people with type 1 diabetes purposely aim for higher blood glucose concentrations before, during and after exercise, in an attempt to prevent hypogly- caemia. A high number of partici- pants started with an elevated blood glucose concentration, which did not delay the start of exercise, and no participant administered extra fast-acting insulin at this point. There was increased hyperglycaemia during exercise in the laboratory,
- 21. which is interesting when also considering the increased hypogly- caemic episodes. This hypergly- caemia increase was also apparent during 8–12 hours after exercise. For the real-life environment, the only increased hyperglycaemia episodes occurred after exercise until 4 hours after the finish. Study limitations The addition of qualitative data would have been useful in clarifying the participants’ experiences of the two environments, which may have explained the outcomes. It could be thought that participants may not have exercised at 70% VO2 max dur- ing the real-life sessions as they were not observed by a researcher. This would explain the increase in hypo- glycaemic episodes during the labo- ratory sessions and not in real-life. However, if this was the case, the participants would not have experi- enced an increase in delayed hypo- glycaemia after the real life sessions. It may also be viewed as more stress- ful running outside due to being aware of the environment and safety issues such as cars, whereas in the laboratory there were no decisions made regarding the route. Another variable which was not accounted for was that of temperature, as hot and cold temperatures could affect gly-
- 22. caemic control. As statistical analysis demon- strated the environment did not affect glycaemic control, this observa- tion must provide reassurance that previous laboratory based research and subsequent findings can be used in patient education to advise on self- management strategies during exer- cising and subsequently clarify the reproducibility of clinical research in everyday life. However, it must be taken into consideration that the sample size was a limitation of this current study and, if correctly pow- ered, results may have been different. Another reason for caution with extrapolating laboratory based statis- tical data would be extreme outliers of hypoglycaemia and hypergly- caemia. In the current study, extreme outliers were not highlighted in the statistical analysis, but the descriptive analysis demonstrated a difference with the patterns of hypoglycaemia and hyperglycaemia in each environ- ment. This remains an important issue for patients, but will require further investigation using a larger sample size. Despite the lack of power in the study, the self-management algo- rithm was modified to reflect the hypoglycaemia episodes; a slight
- 23. increase in the carbohydrate amounts were introduced into the 220 PRACTICAL DIABETES VOL. 32 NO. 6 COPYRIGHT © 2015 JOHN WILEY & SONS Can laboratory based research regarding type 1 diabetes and exercise be applied into the real-life environment? Original article before exercise section, and a carbo- hydrate snack at bedtime was intro- duced into the after exercise section. The findings described cannot be compared with other results in the literature since no studies, as far as these authors are aware, have been published comparing exercise envi- ronments in this manner. Despite this, laboratory findings regarding self-management strategies are used by health care professionals to advise patients on exercise management in daily life, although they have not been evaluated in that environment. Conclusion The initial aim of this study was to determine whether results from lab- oratory based research examining glycaemic control during and after exercise can be applied to a real-life
- 24. (non-laboratory) environment; stat - istical analysis infers that this is acceptable. However, the descriptive analysis does suggest differences within the laboratory environment during exercise, and the delayed risk of hypoglycaemia after the real-life sessions 8–12 hours after the post-exercise insulin dose, as it would appear that there was a difference between environments. Hyper glycaemia frequency is also increased in the laboratory environ- ment during exercise and 8–12 hours after exercise, whereas in real- life the increase was noticed after exercise until 4 hours after the finish of the session. When considering acceptable glucose levels, the real- life environment data do suggest better glycaemic control; however, the larger standard deviations would imply greater variability. These find- ings are essential for patient safety and education, especially regarding the prevention of hypoglycaemia. Nevertheless, it is acknowledged that these differences were observed patterns and thus were not statisti- cally analysed. A larger sample size would be required to make further interpretation and conclusions. However, this does highlight issues when applying laboratory research findings into clinical care.
- 25. Acknowledgments We thank Dr Martin Maxwell for his on-going support, and Spencer Fildes from Nipro Diagnostics UK for providing the TrueResult blood glucose meters. Declaration of interests There are no conflicts of interest declared. References 1. Grimm J, et al. A new table for prevention of hypo- glycaemia during physical activity in type 1 diabetic patients. Diabetes Metab 2004;30:465–70. 2. Peter R, et al. Effects of exercise on the absorption of insulin glargine in patients with type 1 diabetes. Diabetes Care 2005;28(3):560–5. 3. Rabasa-Lhoret R, et al. Guidelines for premeal insulin dose reduction for postprandial exercise of different intensities and durations in type 1 dia- betic subjects treated intensively with a basal- bolus insulin regimen (ultralente-lispro). Diabetes Care 2001;24(4):625–30. 4. West DJ, et al. Blood glucose responses to reduc- tions in pre-exercise rapid acting insulin 24 h after running in individuals with type 1 diabetes. J Sports Sci 2010;28(7):781–8. 5. Bracken RM, et al. Impact of pre-exercise rapid act-
- 26. ing insulin reductions on ketogenesis following running in type 1 diabetes. Diabet Med 2011; 28(2):218–22. 6. Lumb AN, Gallen IW. Insulin dose adjustment and exercise in type 1 diabetes: what do we tell the patient? Br J Diabetes Vasc Dis 2009;9(6):273–7. 7. Perry E, Gallen IW. Guidelines on the current best practice for the management of type 1 diabetes, sport and exercise. Pract Diabetes Int 2009;26(3): 116–23. 8. American Diabetes Association. Diabetes mellitus and exercise. Diabetes Care 2002;25(1):64–8. 9. Ertl AC, Davis SN. Evidence for a vicious cycle of exercise and hypoglycaemia in type 1 diabetes mellitus. Diabetes Metab Res Rev 2004;20:124–30. 10. Gallen I. Helping the athlete with type 1 diabetes. Br J Diabetes Vasc Dis 2004;4:87–92. 11. Riddell M, Perkins B. Type 1 diabetes and vigorous exercise: applications of exercise physiology to patient management. Can J Diabetes 2006;30(1): 63–71. 12. Evans M. The role of the real world data in clinical practice. Diabetes Update 2014;Autumn:14. 13. Potteiger JA. ACSM’s introduction to exercise science. Philadelphia: Lippincott Williams & Wilkins, 2010. 14. Dose Adjustment For Normal Eating (DAFNE) Study Group. Training in flexible, intensive insulin man-
- 27. agement to enable dietary freedom in people with type 1 diabetes: dose adjustment for normal eating (DAFNE) randomised controlled trial. BMJ 2002; 325(7367):746. PRACTICAL DIABETES VOL. 32 NO. 6 COPYRIGHT © 2015 JOHN WILEY & SONS 221 Can laboratory based research regarding type 1 diabetes and exercise be applied into the real-life environment? Original article l Most exercise and type 1 diabetes research has been performed in a laboratory environment l Apart from case studies, no publications have been found regarding self-management and glycaemic control observing patients in real-life environments l Statistical analysis did not show a difference on the effect of glycaemic control in a laboratory environment compared to real-life l Descriptive analysis did show differences especially in relation to hypoglycaemic episodes during the exercise period and overnight l No major conclusions can be made from these findings as the study was underpowered, but it does highlight issues to consider when using laboratory data in clinical practice Key points
- 28. Find out how non-diabetes drugs impact diabetes patients. Visit the Practical Diabetes website and click on drug notes Drug notes Aliskiren l Amlodipine l Bisoprolol l Bromocriptine l Bumetanide l Carbamazepine l Cilostazol l Clopidogrel l Colesevelam l Dabigatran l Darbepoetin alfa l Diazoxide l Digoxin l Dipyridamole l Domperidone l Doxazosin l Dronedarone l Duloxetine l Eplerenone l Erythromycin l Ezetimibe l Gabapentin l Indapamide l Ivabradine l Labetalol l Lidocaine l Lorcaserin l Losartan l Methyldopa l Metoclopramide l Nicorandil l Nifedipine l Omacor l Orlistat l Prasugrel l Prolonged-release nicotinic acid l Quinine sulphate l Ramipril l Ranolazine l Rimonabant l Rivaroxaban l Rosuvastatin l Sibutramine l Spironolactone l Tadalafil l Testosterone l Torcetrapib www.practicaldiabetes.com Copyright of Practical Diabetes is the property of John Wiley & Sons, Inc. and its content may not be copied or emailed to multiple sites or posted to a listserv without the copyright holder's express written permission. However, users may print, download, or email articles for individual use.