Download to read offline
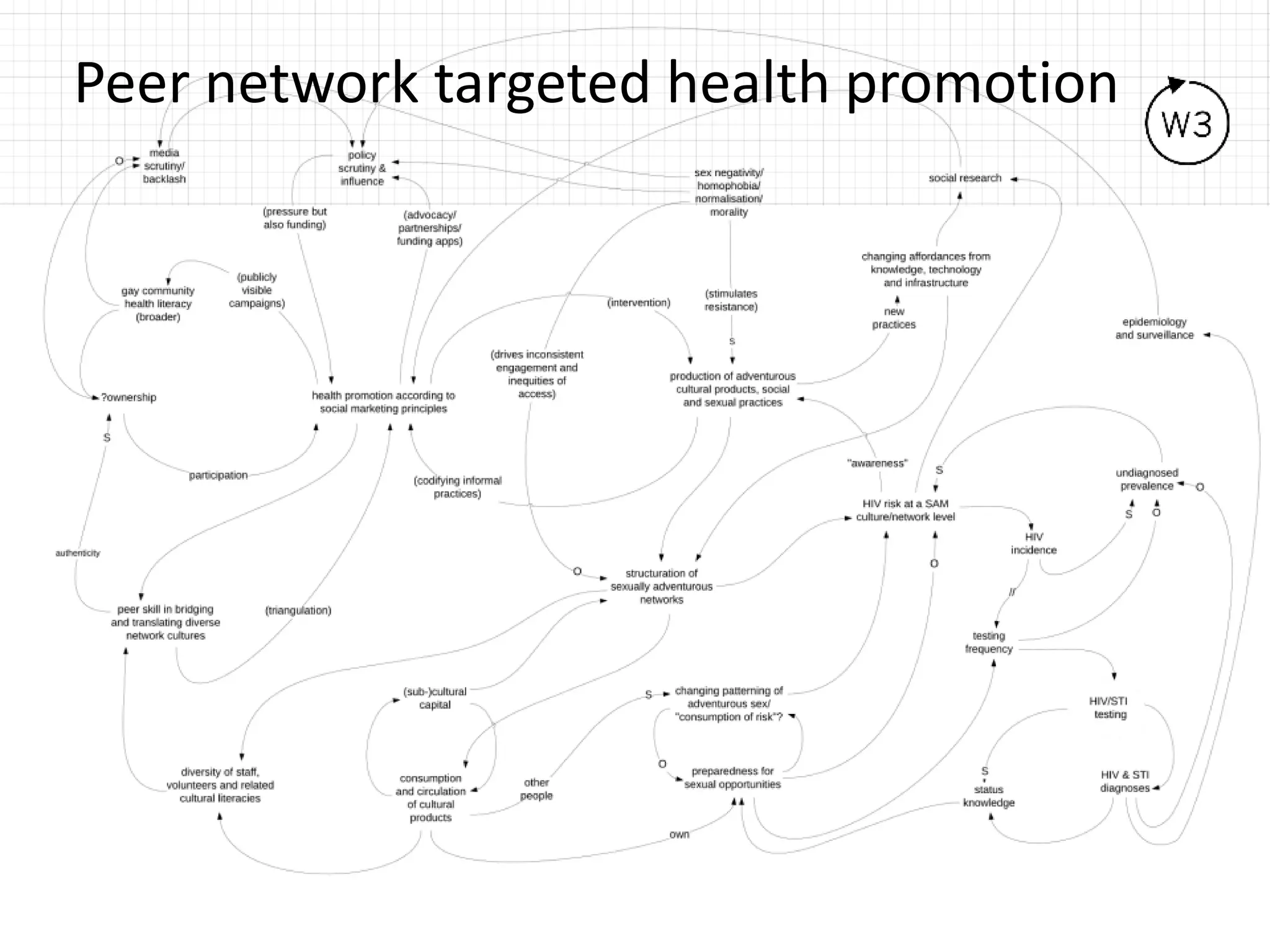
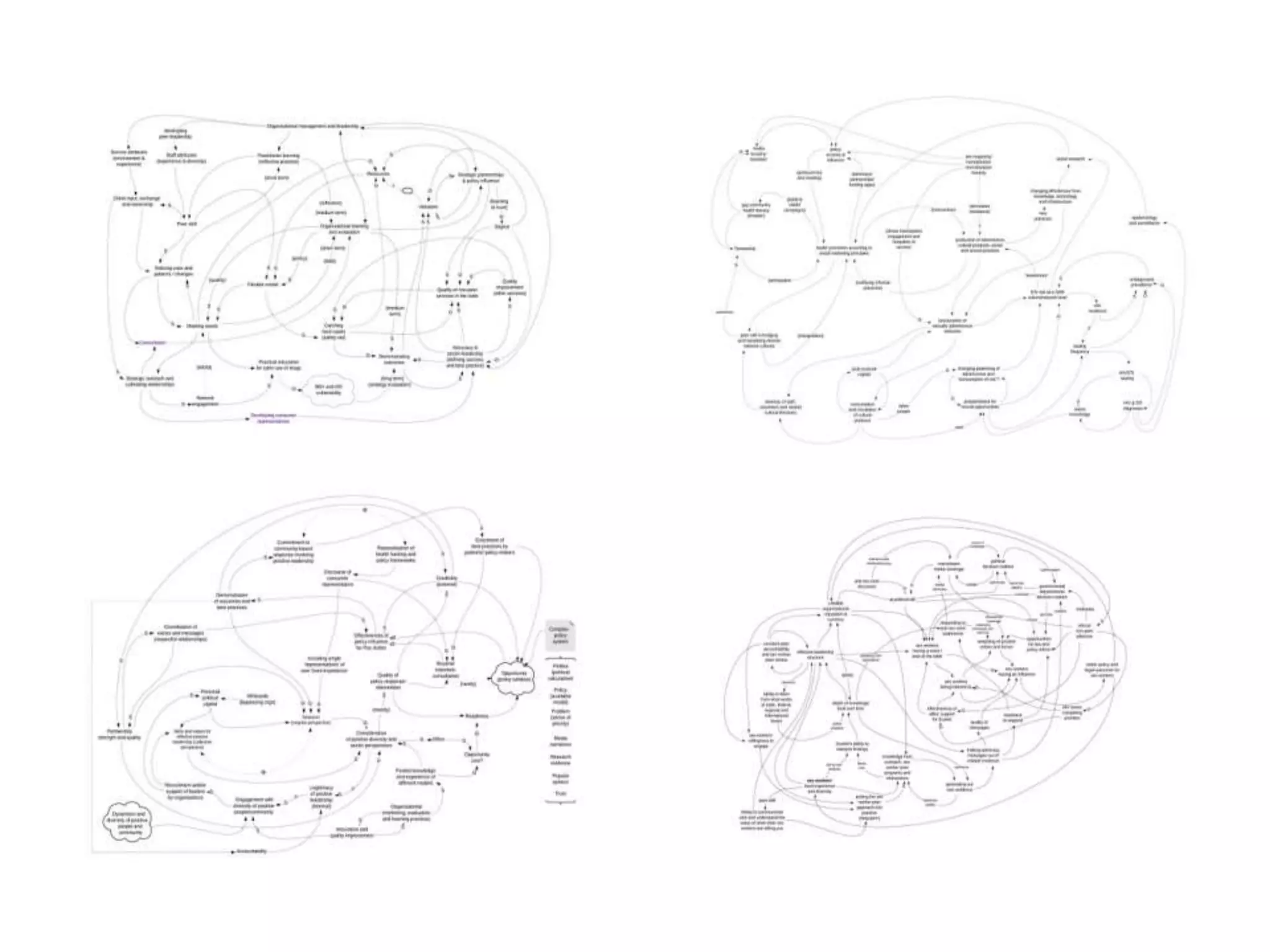
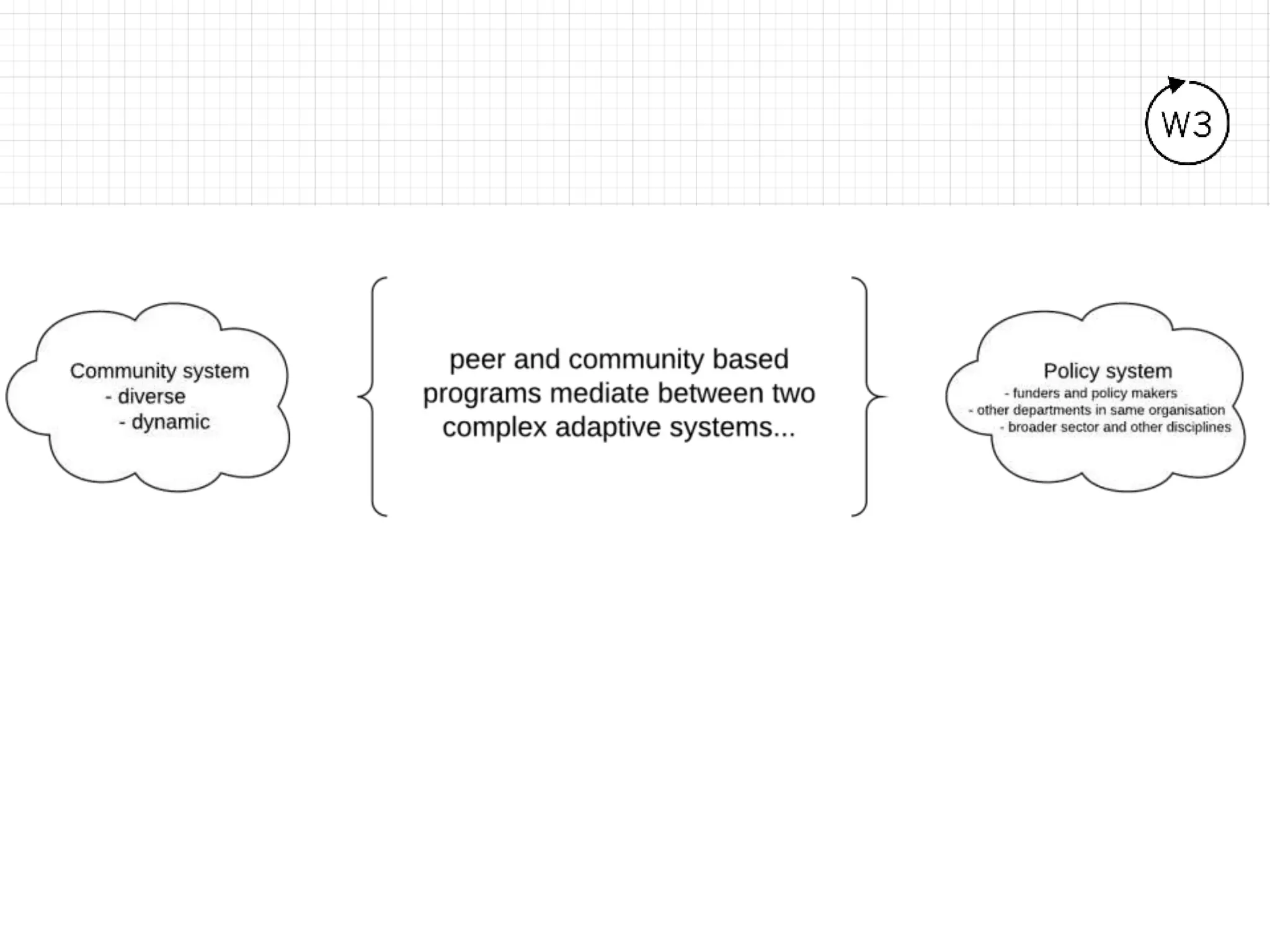
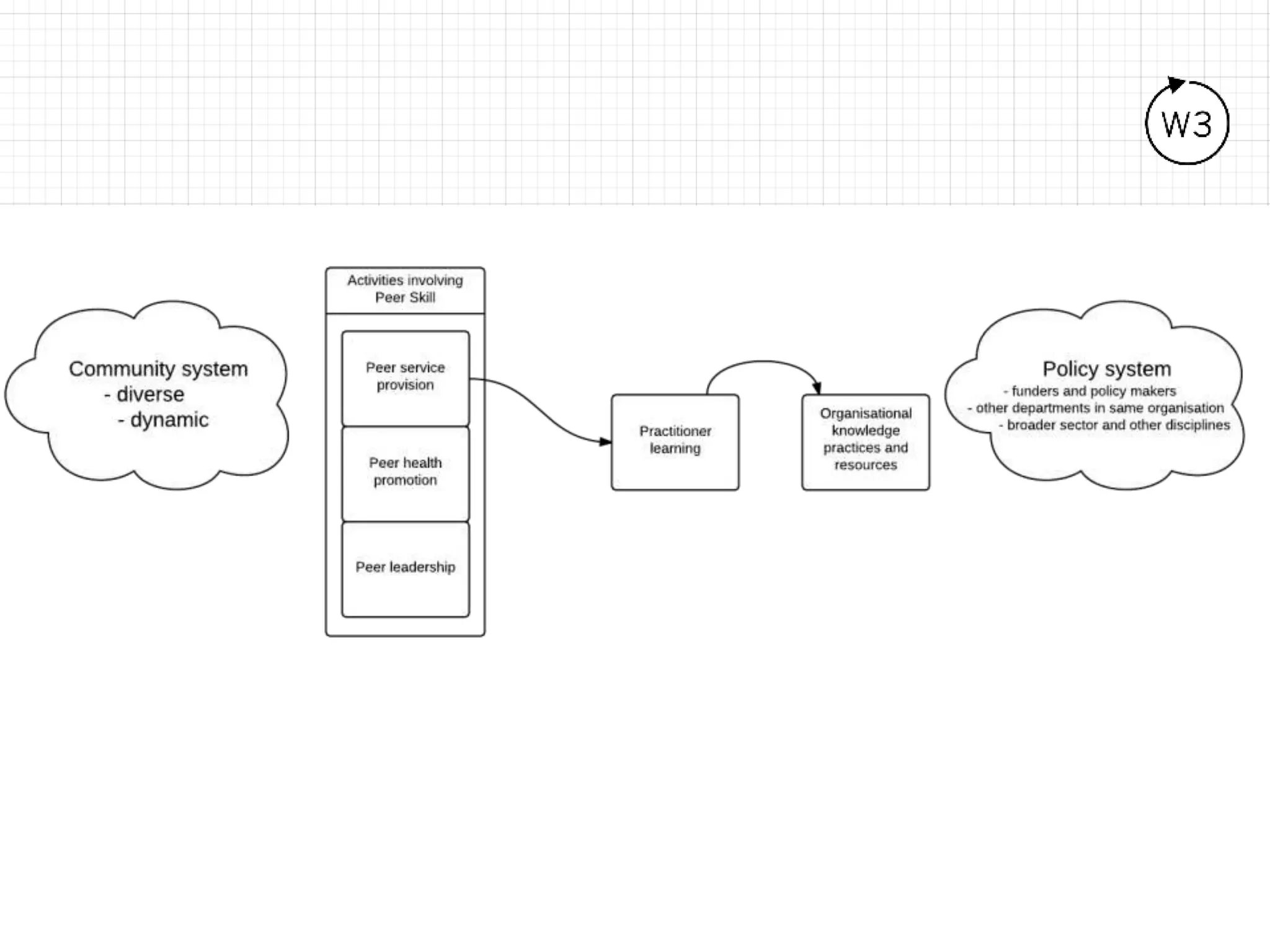
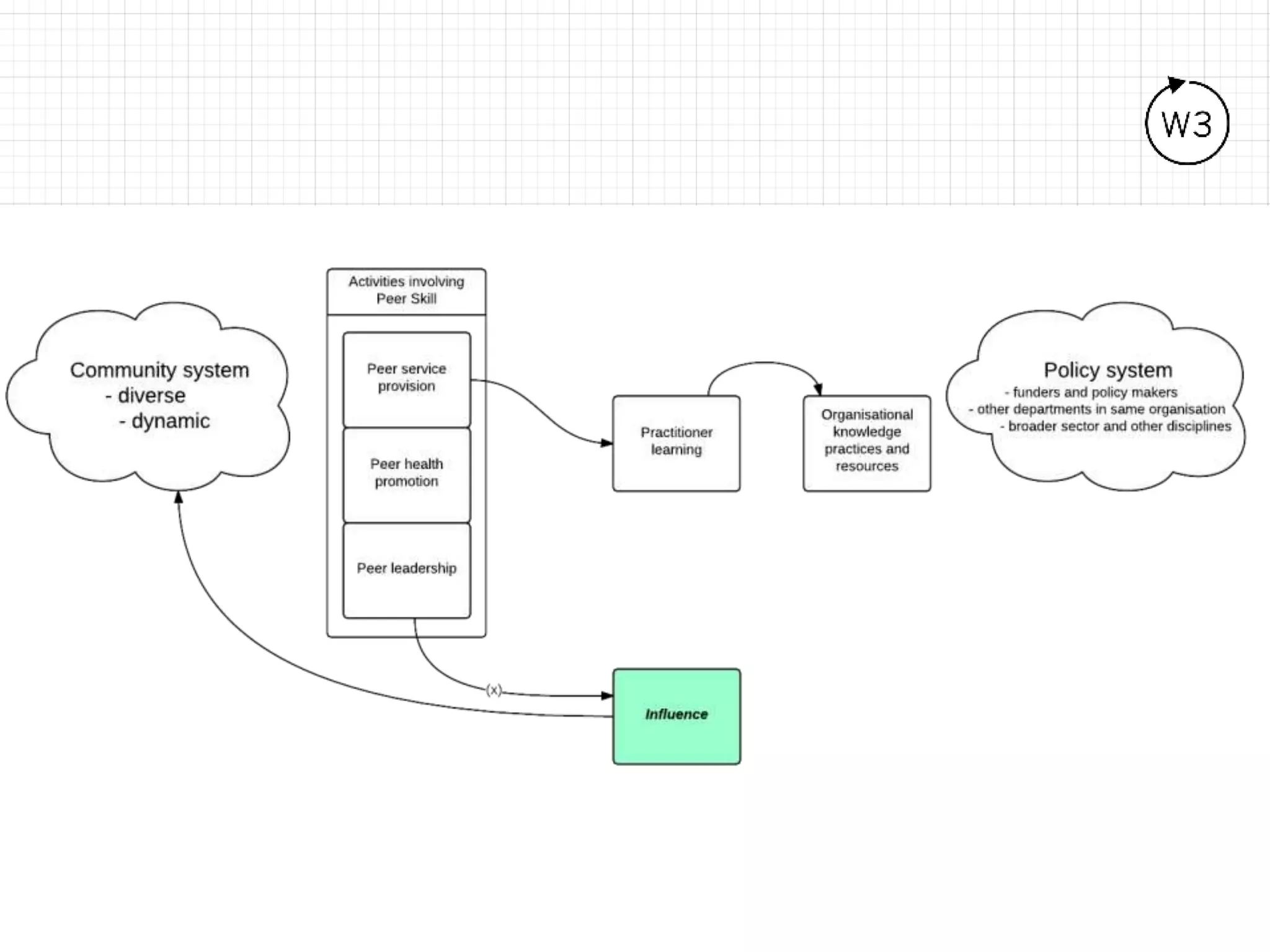
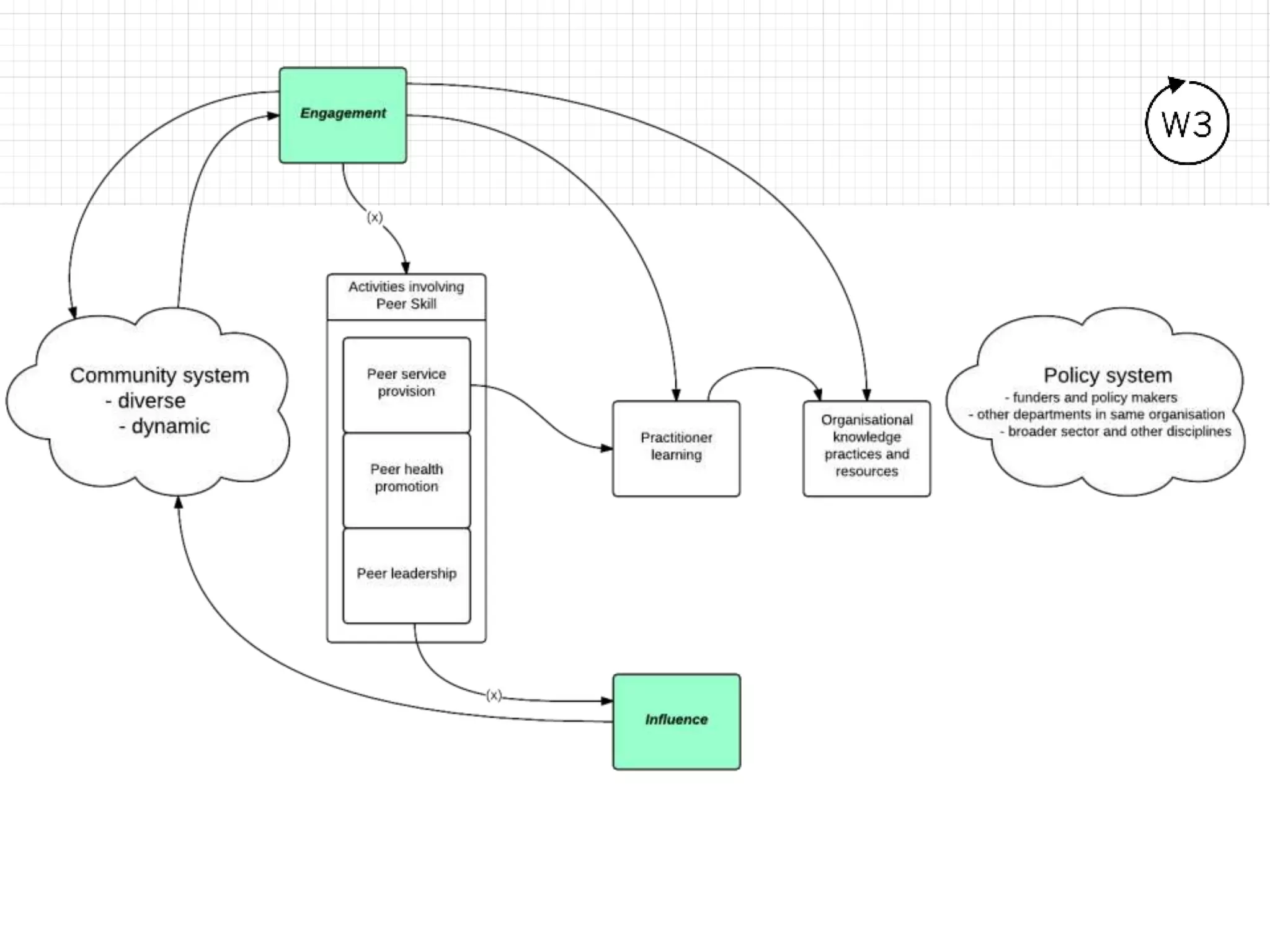
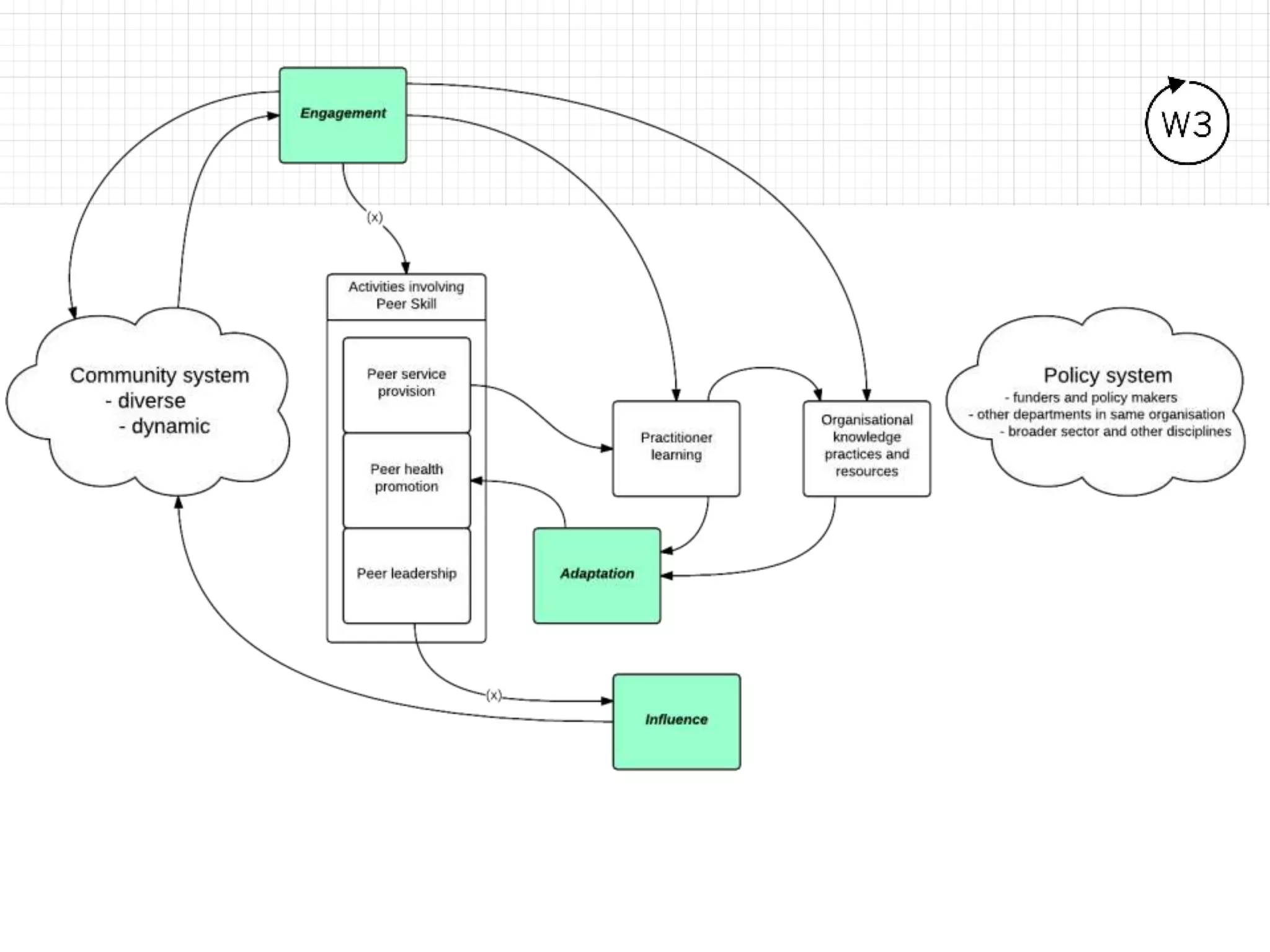
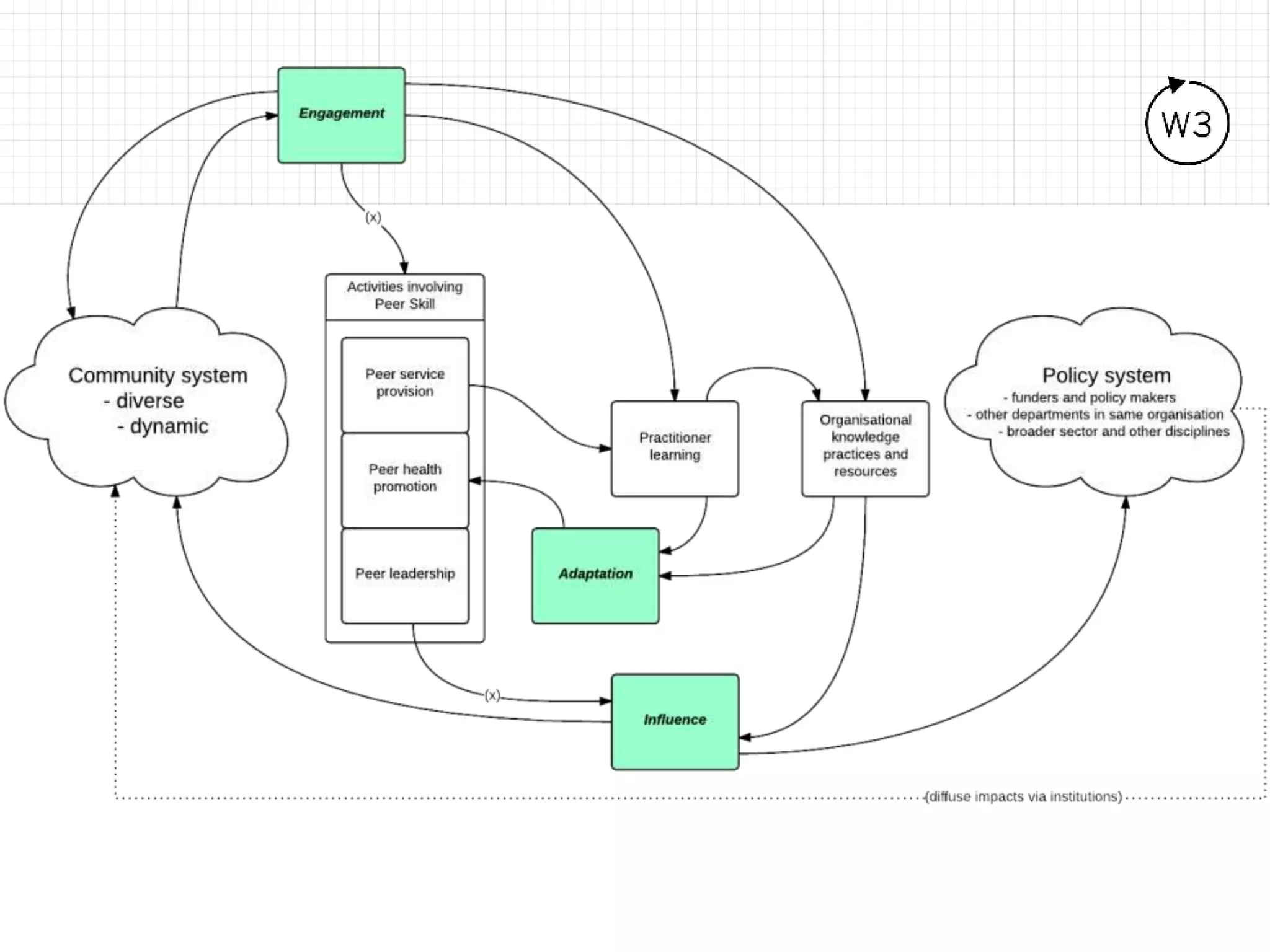
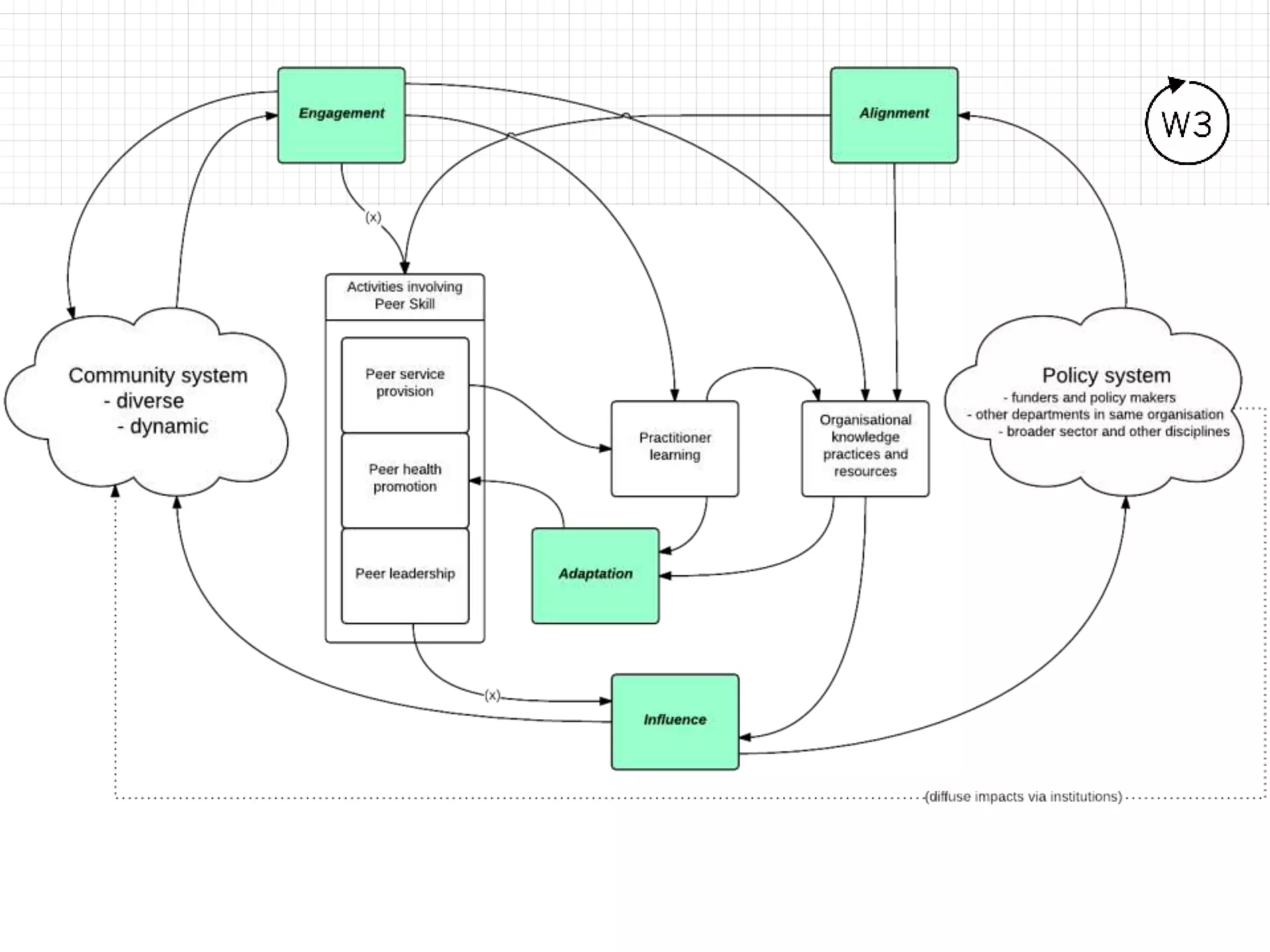
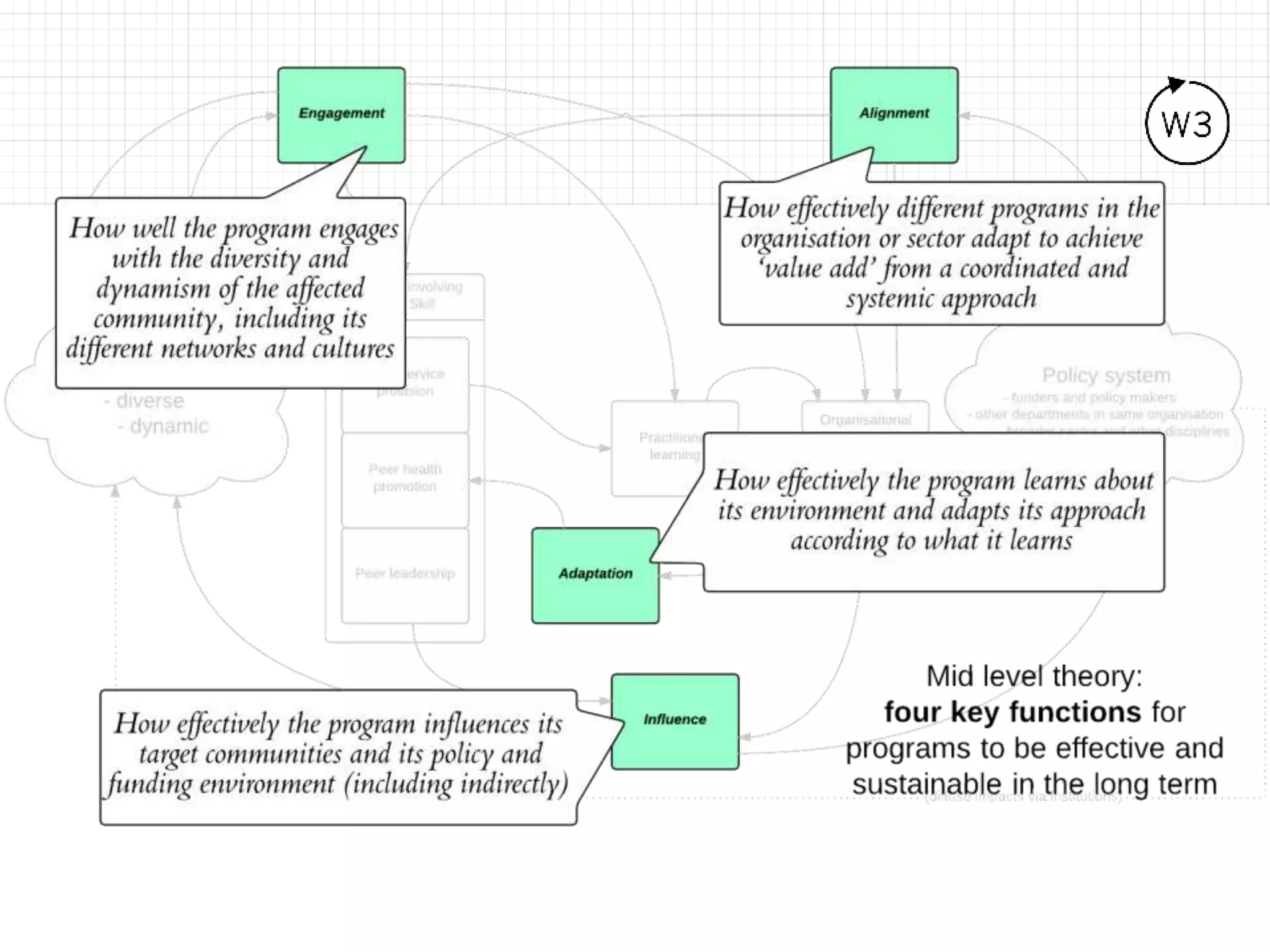
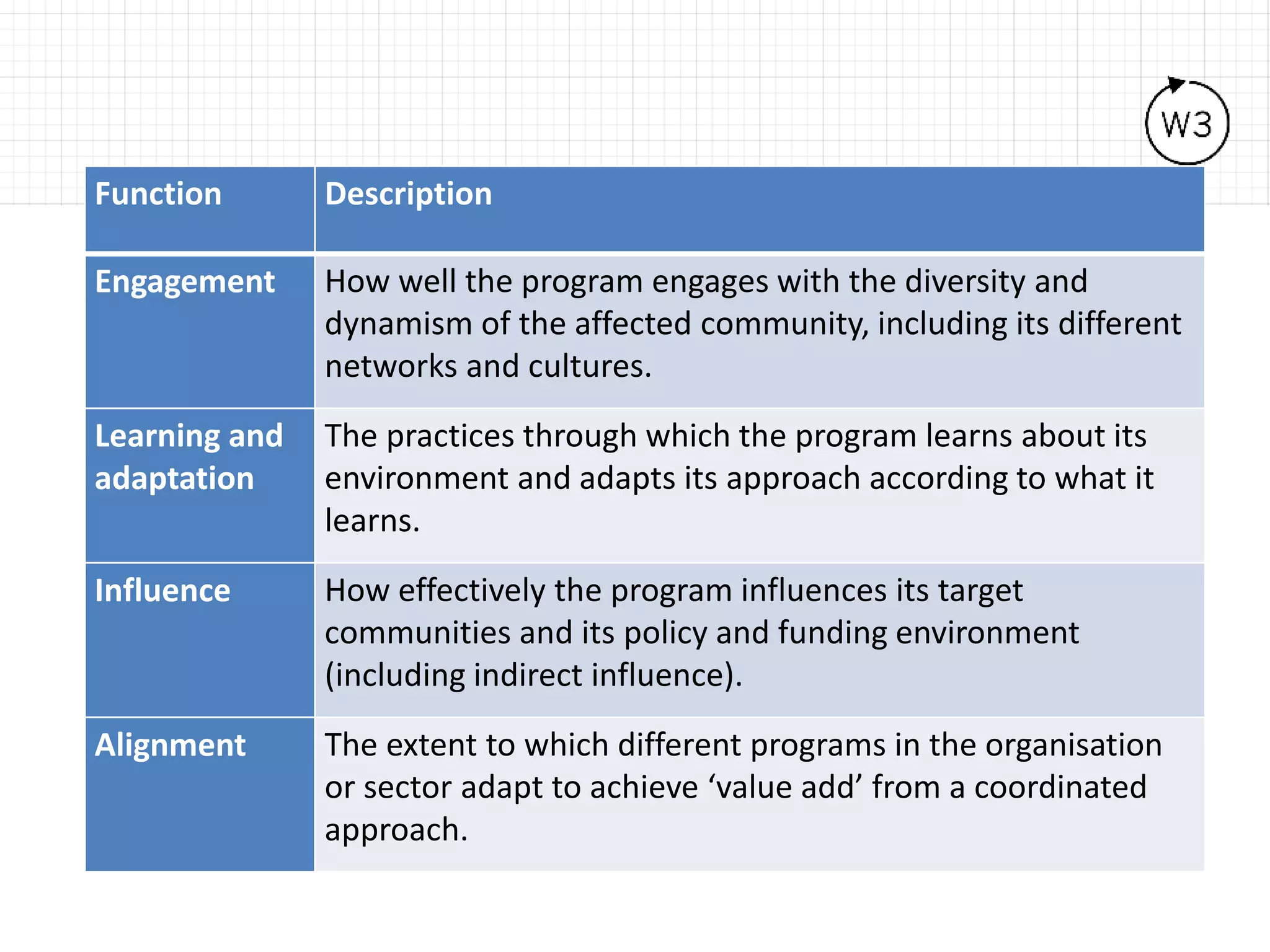

This document discusses using systems approaches to better understand peer-based programs for HIV and HCV. It summarizes work done with various organizations representing people who use drugs, gay men, people living with HIV, sex workers, and others. Systems approaches were used to develop more sophisticated theories of how peer-based programs work and influence communities. System dynamics maps showed how interventions engage with communities. Key functions and draft indicators were identified to demonstrate influence and help programs evaluate their work and influence on communities and policies. The document provides an overview of the Understanding What Works & Why (W3) project which aims to help answer questions about program influence and effectiveness using systems approaches.






























































































