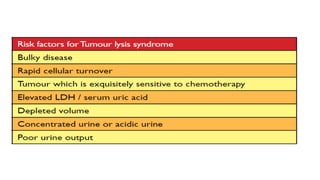
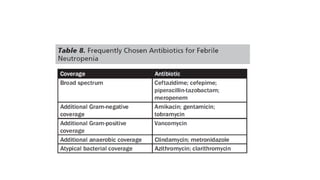
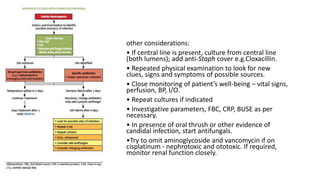
This document outlines several oncological emergencies including tumor lysis syndrome, hyperleukocytosis, disseminated intravascular coagulopathy, superior vena cava obstruction, febrile neutropenia, and infection. It provides details on the characteristics, risks factors, signs and symptoms, and management approaches for each emergency. Key aspects of management include hydration, monitoring of electrolytes and blood counts, use of allopurinol or steroids to prevent tumor lysis, platelet transfusions for coagulopathies, and early treatment of febrile neutropenia with antibiotics. The document emphasizes the need for prompt recognition and treatment of these potentially life-threatening oncological complications.



![ONCOLOGICAL EMERGENCY BY DR AISHA KABIR TURAKI [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/oncologicalemergencybydraishakabirturakiautosaved-240718152317-4bc93696-thumbnail.jpg?width=640&height=640&fit=bounds)














































