Downloaded 45 times
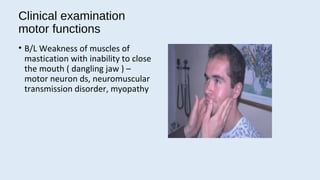
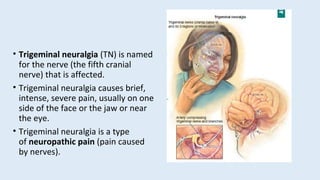
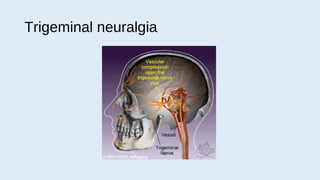


The trigeminal nerve is the largest and most complex cranial nerve, with both sensory and motor functions. Trigeminal neuralgia causes severe, stabbing, intermittent facial pain and is caused by compression or irritation of the trigeminal nerve. Symptoms include episodes of unilateral pain in the face, mouth, or eye that are triggered by mundane activities like eating or talking. Diagnosis is clinical without a confirmatory test. Treatment involves drug therapy with anticonvulsants or surgical procedures like microvascular decompression to relieve nerve compression.























































































