Downloaded 103 times

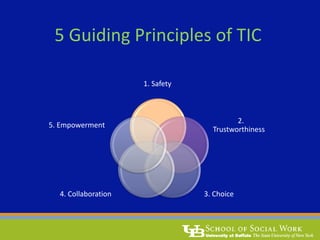
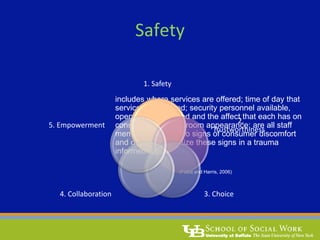
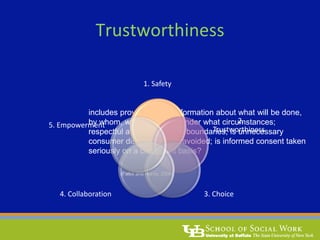
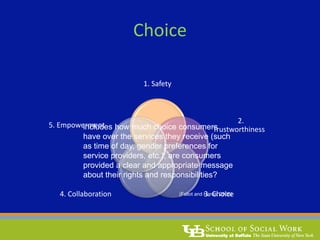
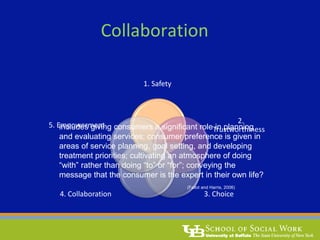
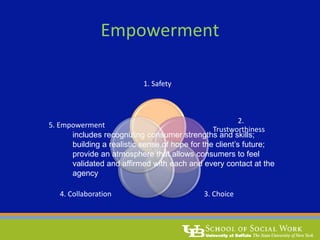


The document discusses trauma-informed social work, emphasizing the prevalence of traumatic experiences among individuals seeking social work services and the importance of trauma-informed care (TIC) in service delivery. TIC focuses on understanding trauma reactions, avoiding inadvertent retraumatization, and creating an environment that promotes safety, trust, choice, collaboration, and empowerment for survivors. It also outlines the impacts of trauma and the necessity for systematic changes in service provision to better support affected individuals.

































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)






![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)










