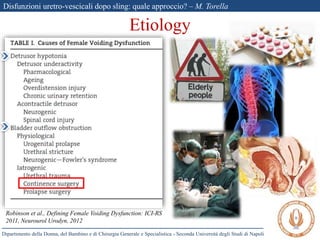
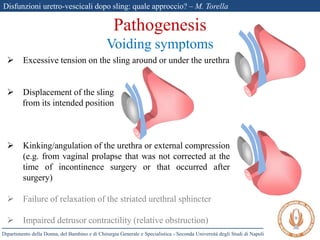
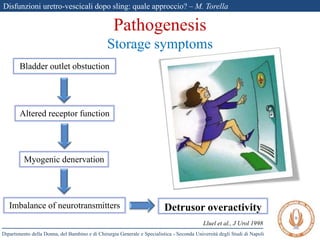
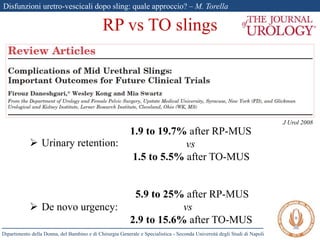
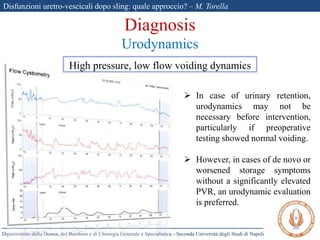
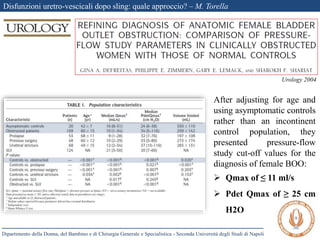
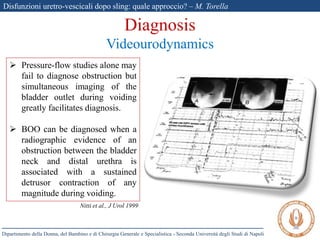
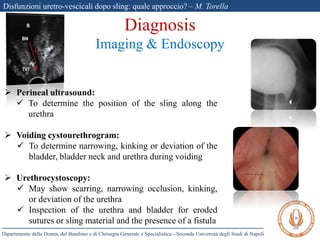
The document discusses voiding dysfunctions after sling surgery for stress urinary incontinence. It notes that voiding dysfunctions occur in 2-20% of patients after various sling procedures. The causes can include excessive tension on the sling, displacement of the sling, or external compression of the urethra. Diagnosis involves evaluating the patient history and symptoms, as well as urodynamics testing and imaging exams. Treatment options include conservative measures like clean intermittent catheterization, or surgical interventions like sling loosening or incision if conservative options fail. Early sling loosening or incision within 2 weeks of surgery appears to effectively resolve voiding dysfunction in many patients without compromising continence.