Definition
• The term“tissue engineering” as it is nowadays used was
introduced in1987.
• “Tissue Engineering is the application of the principles
and methods of engineering and life sciences toward the
fundamental understanding of structure-function
relationships in normal and pathologic mammalian
tissue and the development of biological substitutes to
restore, maintain, or improve function.”
3.
Definition
• Regenerative Medicine- "process of replacing,
engineering or regenerating human or animal cells,
tissues or organs to restore or establish normal
function".
• This field holds the promise of engineering damaged
tissues and organs by stimulating the body's own repair
mechanisms to functionally heal previously irreparable
tissues or organs
4.
The goal
• Toassemble functional constructs that restore,
maintain, or improve damaged tissues or whole organs.
• Growth of cell in three dimensional systems
• Delivery systems for protein therapeutics
• Cell cultivation methods for culturing recalcitrant cells
• Transgenic protein expression in transplantable cells
• Vehicles for delivering transplantable cells
• Avoiding immunogenicity in transplantation systems
• Development of markers for tracking transplanted cell
• Developing in vivo and ex vivo biosensors for monitoring
cell behaviour during tissue production.
5.
Tissue engineering
• Tissuescan be viewed as a composite of:
1.cells (both parenchymal and stromal)
2.matrix and
3.blood vessels.
• Cell maintenance and behavior including growth and
regeneration are influenced by biochemical and
biomechanical interplay.
• The development of a functional tissue must be
vascularized to ensure survival of the neotissue.
• Each of these components is the purview of the tissue
engineer.
Cell sources fortissue engineering
• Cells used for TE,
⚬Autologous - preferred due to the lack of immunogenicity
⚬Heterologous,
⚬Xenogeneic and each type may be
■ mature differentiated
■ precursor stem cell form.
8.
Cell sources fortissue engineering
• Chondrocytes for cartilage
• Osteocytes for bone
• Schwann cells for nerves
• Fibroblasts for ligament and tendon engineering
⚬ All these have significant proliferative potential in vitro
• Adult cardiomyocytes, hepatocytes, and adipocytes
⚬Challenge - difficult to culture and expand in vitro
9.
Cell sources fortissue engineering
• A second challenge
⚬Collection of cells – biopsy; uncomfortable and
impossible due to diseased state of the tissue
• Solution
⚬Utilize stem cells; expanded and differentiated ex vivo.
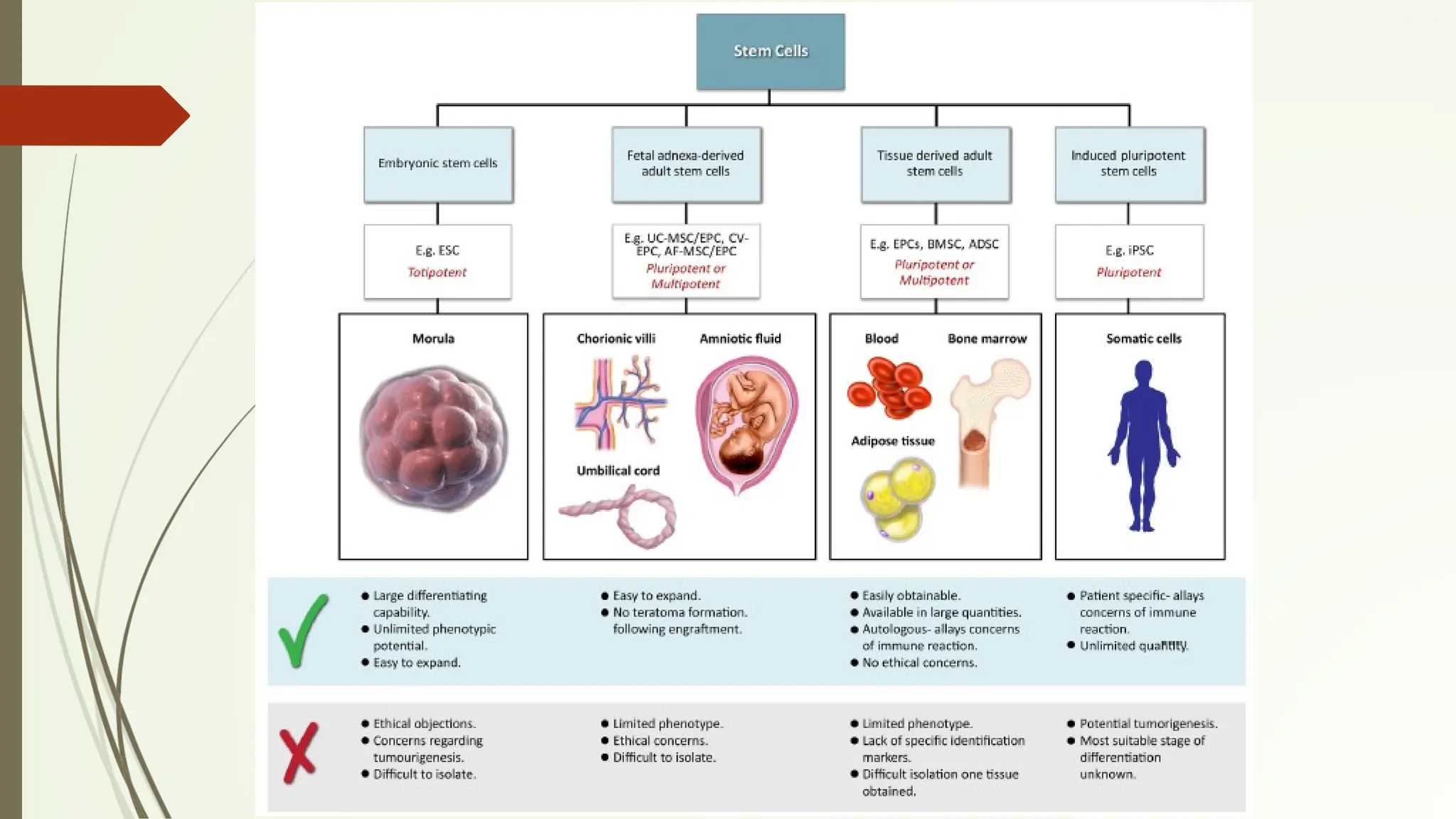
• Multiple types of stem cells exist
⚬E.g. embryonic, adult, and induced pluripotent stem
cells.
• Discuss embryonic stem cells
• Focus on stem cell types most relevant to the plastic
surgeon; sources of cells, advantages and disadvantages,
use in TE
Embryonic stem (ES)cells
• Totipotent
• Infinitely proliferative
• Differentiate into all tissue types
• Are also unstable and form teratomas
• Ethical and legal concerns - sourcing and utilization
• Successful differentiation protocols have been found to induce ES
cells along specific lineage pathways from all germ layers towards
many specific tissues and organs.
• These cells are probably immunogenic and ethical issues will persist.
• Regulatory and organizational issues
12.
Adult stem cells
•Multipotent
• Limited in their proliferation capacity and differentiation
potential.
• Collected and expanded from tissue biopsies through a
process referred to as the colony forming unit (CFU) assay
• Adult stem cells in bone marrow:
⚬Hematopoietic stem cells (HSCs), which differentiated into the
white blood cell population and
⚬Mesenchymal stem cells (MSCs),
■ Progenitors of bone, cartilage, fat, and muscle.
■ Endothelial progenitor cells (EPCs) have been isolated and
cultured from adult peripheral blood.
13.
Adult stem cells
•MSCs and EPCs also present in fat tissue associated with
the microvasculature
⚬Known as adipose-derived stem cells (ASCs).
• Relevant stem cells in Plastics
⚬Mesenchymal stem cell
⚬ Adipose-derived stem cell
⚬Endothelial progenitor cell.
14.
Mesenchymal stem cells
•Do not express MHC class II markers
• Showed to be immune-privileged and may be used as
allografts.
15.
Mesenchymal stem cells
•Paracrine-growth factor hormonal- cytokine immune-
modulatory effects probably account for the benefits seen
with these stem cells.
⚬ E.g., Ischemia increases homing of these cells to the injured
site
■ MSCs release high levels of vascular endothelial growth factor
(VEGF)
■ This modulates the repair of capillaries.
⚬MSCs injected intravenously in cardiac infarct models do not
implant in the heart nor become heart tissue
■ Lodge in the lung
■ Activated to secrete the anti-inflammatory protein TSG-6
■ Probably the anti-inflammatory factor that induces the
beneficial effects.
16.
Adipose-derived stem cells
•Abundant
• Ease of harvest by liposuction
⚬ Preferred autologous stem cell source
• Similar properties to bone marrow-derived stem cells
• More easily cultured
• Grows more rapidly
• Cultured for longer periods than bone marrow stem cells
before senescence
• Richer source of stem cells
⚬ One gram of adipose tissue can yield 5000 stem cells
• ASC population may also have low immunogenicity
17.
Endothelial progenitor cells
•Incorporation of a functional vasculature network in the neotissue is
important
• Endothelial progenitor cell (EPC) most promising
• First identified in 1997 by Asahara et al.,
• Present in adult circulation
• Isolated and expanded from peripheral blood collected through
simple venipuncture.
• Two distinct EPC populations that participate in vascular repair and
angiogenesis via different mechanisms.
⚬ Circulating angiogenic cells (or colony forming unit–Hill cells) – support
via paracrine signalling
⚬ Endothelial colony forming cells (ECFCs) – regenerate an endothelial
population
18.
Challenges associated withadult stem
cells
• Advantages
⚬An autologous and/or non-immunogenic source of
cells.
• Limitations
⚬Patient-to-patient variations in their prevalence,
proliferative capacity, and differentiation potential
⚬ Additionally, their utility is also a factor of age and
disease state of the donor
⚬ Exit the cell proliferation cycle (prematurely senesce)
or prematurely lose differentiation potential during
ex vivo expansion
Schipper B, Marra K, Zhang W, et al. Regional anatomic and age effects on cell function of human adipose-derived
stem cells. Ann Plast Surg. 2008;60:538–544
19.
Induced pluripotent stemcells (iPS)
• Unlimited proliferation capacity
• Ability to differentiate into cells from all germ layers both in
vitro/vivo
• Major problem - Requires genetic manipulation of the cells
⚬ Two of the genes used in this process (c-Myc and KLF4) are oncogenes
• Zhou et al. (2009) delivered the 4 proteins that the above-
mentioned genes code for directly into the cell
⚬Protein-induced pluripotent stem cells (piPSCs)
⚬Bypasses the need for viral or plasmid transfection and reduces
the risks of cancer formation.
⚬Drawback - efficiency of the protein induction is very low
Takahashi K, Yamanaka S. Induction of pluripotent stem cells from mouse embryonic and adult fibroblast cultures by defined factors. Cell (2006) 126(4):663–
76. doi:10.1016/j.cell.2006.07.024
20.
Induced pluripotent stemcells (iPS)
• Challenge
⚬Not immune privileged requiring collection, induction,
expansion, and differentiation of autologous cells.
⚬Costly and time-consuming
• Solution
⚬Create a bank of iPS cells that can be HLA matched to the
patient
21.
Cellular interactions withtheir
environment
• Many cell types are exquisitely sensitive to stimuli present in
the environment.
• Stimuli include;
⚬Soluble molecules
⚬Molecular recognition sites present in the solid phase
(ECM or biomaterial)
⚬Interactions with other cells
⚬Substrate stiffness and the micro/nanostructure of the
surroundings
22.
Soluble signals
• Solublebiomolecules eg Metalloproteins
Growth factors
Chemokines
Play vital roles locally and systemically in repair and tissue
development.
• Understand the appropriate soluble signaling molecules
⚬to maintain cell viability both during culture and in vivo,
⚬ to maintain cellular phenotype,
⚬to drive lineage specific differentiation of stem cells
23.
Matrix signals
• Cellsalso possess receptors such as integrins and
syndecans that bind to a variety of ligands present in the
extracellular matrix (ECM)
• Many cell types are adhesion dependent
• Also the number and strength of bonds with the external
matrix affects a wide variety of cellular behaviors ranging
from adhesion, focal adhesion formation and migration to
morphology.
• Additionally, the ECM binds and sequesters growth factors
that also drive cellular function.
24.
Intercellular signals
• Cellsalso interact with neighboring cells in both native tissue and in ex
vivo culture
• Two main methods: >Direct contact via receptors such as cadherins
>Soluble signaling through paracrine factors
• In traditional cell culture, single populations of cells are grown in
isolation, implanted and rely on recruitment of supporting cellular
structures and matrix to evolve into a stable, functional tissue
• However, co-culturing cells with other types prior to implantation can
facilitate their survival and function. E.g.
⚬Endothelial cells for vasculature
⚬MSCs for paracrine effects or for their ability to incorporate into
developing tissues in vivo like blood vessels
⚬Beating cardiomyocytes with ASCs in vitro to differentiate into
cardiac lineage
25.
Mechanics and structureof the environment
• Cells respond to the mechanical properties and
dimensionality of their environment.
• Response of cells to environmental stiffness and
dimensionality is a tool that can be used to direct cell
function.
⚬E.g. chondrocytes change morphology and lose their chondrogenic
capacity in 2D monolayer culture but can maintain these features
in 3D culture
• Uses;
⚬Distraction osteogenesis
• Periods of stretch promote proliferation and migration
• Relaxation incites cells to cluster together and terminally
differentiate into bone
26.
Mechanics and structureof the
environment
• 3D cultures on biomaterial supports such as
⚬Porous scaffolds
⚬Hydrogels
⚬Microspheres
■ Under conditions designed for the desired cell attachment,
migration, proliferation, and differentiation
• Development of new biomaterials with tailored properties
• Direct the fabrication of these materials into three-
dimensional scaffolds to maximize the healing process
27.
Biomaterials used intissue engineering
• Components of solid tissues
⚬Cells
⚬Extracellular matrix - structure and biochemical signals to the
cells
• When cells are expanded outside the body, they grow in
monolayers, not the intricate patterns of a fully realized 3D
tissue
• Thus, cells are seeded onto a 3D scaffold
⚬Biomaterial scaffolds can be thought of as artificial ECMs
29.
Biomaterials used intissue engineering
• Early tissue engineering used known materials.
⚬Polymers used in degradable sutures
⚬Natural materials such as coral, alginate and collagen.
• Recently, numerous alternatives have been formulated
• Biomaterials for TE
⚬Naturally occurring in the body
⚬From other natural or synthetic sources
⚬Ceramics
⚬Polymers
⚬Hydrogels
⚬Composites of these
⚬Decellularized tissues
30.
Biomaterials used intissue engineering
• The physical form of biomaterials can also vary to suit the
application
⚬Solid materials
⚬Porous scaffolds
⚬Microspheres
⚬Hydrogels
⚬Injectable materials that may cross-link in situ etc.
• Simplicity - facilitate regulatory approval and translation
into clinical application
• Selection depends on the specific requirements of the
tissue being targeted
31.
Biodegradable materials
• Mostare biodegradable, to be replaced by neotissue
• Rate of degradation and loss of integrity will depend on;
⚬Type of biomaterial
⚬Site of implantation
⚬Properties of the biomaterial construct such as surface
area to volume ratio, size, and surface chemistry
• Challenges - Prevention of sudden loss of physical integrity
- Rapid degradation - excessive concentrations
of the
degradation products and can cause adverse
tissue
reactions.
32.
Natural biomaterials
• Chemicallysimilar or identical to molecules in the body
• Readily degraded in vivo
• Interact with cells on a molecular level
• Difficult to obtain and purify
• Vary in properties between batches
• Difficult to sterilize
• Alter their properties during storage,
• Elicit significant immunogenic responses.
33.
Natural biomaterials
Examples;
• Proteins(e.g., collagen, gelatin, silk)
• Polysaccharides (e.g., chitosan, hyaluronic acid)
• Polynucleotides
• Extracts of ECM components
• Increased interest - Decellularized extracellular matrix
(dECM)
⚬In decellularization, cells are removed from allografts or
xenografts to reduce immunogenicity but much of the
complex composition and architecture of the ECM may be
retained
34.
Decellularization is theprocess used in biomedical engineering to isolate the
extracellular matrix (ECM) of a tissue from its inhabiting cells, leaving an ECM
scaffold of the original tissue.
35.
Polymeric biomaterials
1. Hydrophobicpolymers
• Biodegradable polymers that could be used in TE
⚬The polyesters
■ poly(glycolic acid) (PGA)
■ poly(lactic acid) (PLA)
■ poly(ε-caprolactone) (PCL)
■ and their copolymers such as poly(lactide-co-glycolide) (PLGA)
• Mechanical strength & degradation rate – altered by
changing the polymer properties (molecular weight,
composition, molecular architecture, crystallinity,
hydrophobicity)
36.
Polymeric biomaterials
2. Hydrogels
•Water-swollen cross-linked polymer networks which can
absorb up to thousands of times their dry weight of water.
• Advantage of being more like most natural tissues and
allowing mass transport to and from cells.
• Naturally derived
⚬Collagen
⚬Gelatin
⚬Hyaluronic acid
⚬Alginate
• Synthetic
⚬Poly(ethylene glycol) (PEG)-based polymers
37.
Ceramic biomaterials
• Ceramicbiomaterials are primarily utilized in tissue
engineering of hard tissues.
• Calcium phosphates, such as hydroxyapatite, and bioactive
glasses have been developed as bioceramics for bone
tissue engineering.
• Characteristics
⚬Bioceramics are brittle but have high compressive strength,
can bond strongly to bone, and can be osteoinductive.
38.
Advanced biomaterials fortissue
engineering
1. Tailored delivery systems
• Growth factors, anti-inflammatory peptides, and drugs may
be incorporated into biomaterial delivery vehicles for
release at the desired time during tissue development.
• Release systems are designed to deliver multiple molecules
over different timescales via continuous or pulsatile
delivery, which may be programmed or triggered by some
change in the local environment.
• Fabricated from biodegradable polymers in the form of
⚬ micro or nanoparticles
⚬ capsules,
⚬ within walls/surfaces of scaffolds or hydrogels
39.
Advanced biomaterials fortissue
engineering
2. Smart Polymers
• Changes in environmental conditions - changes to the
molecular conformation of many materials.
• Environmentally-induced changes may be harnessed, thus
smart polymers.
• Used to >encapsulate and release payloads of cells or drugs,
>form gels upon injection in vivo
>for cell sheet engineering.
• Example - Thermo-responsive polymer N-
isopropylacrylamide (NIPAM)
• Used to grow confluent cell sheets and then to detach the
intact sheet along with the ECM that the cells have
deposited.
40.
Advanced biomaterials fortissue
engineering
3. Non Fouling Materials
• Successful strategies - use of chemical surface
modifications
• Initial stage of FBR is the adsorption of a complex layer of
biomolecules from body fluids that can be denatured and
lead to an immune reaction.
• Non-fouling materials (or stealth materials) resist the
adsorption of these proteins.
• New generations of non-fouling materials - active area of
research
⚬Zwitterionic polymers
⚬Mixed charged polymers
⚬Polyoxazolines
41.
Advanced biomaterials fortissue
engineering
4. Biofunctionalized materials
• Is based on a “blank slate” from the non fouling
materials/surfaces.
• Decorated with bioactive molecules, through covalent
immobilization.
• These biofunctionalized materials interact with receptors
on the cell surface and drive cellular behavior with
biological specificity.
• Most common strategy - materials with ligands that engage
specific integrin receptors.
• Thus, only cells that express the appropriate integrin are
able to adhere to the material.
42.
Tissue engineering constructs
•These biomaterials are fabricated into a tissue scaffold to
support regeneration.
• Structures
⚬Porous scaffolds and hydrogels
⚬Meshes or microspheres
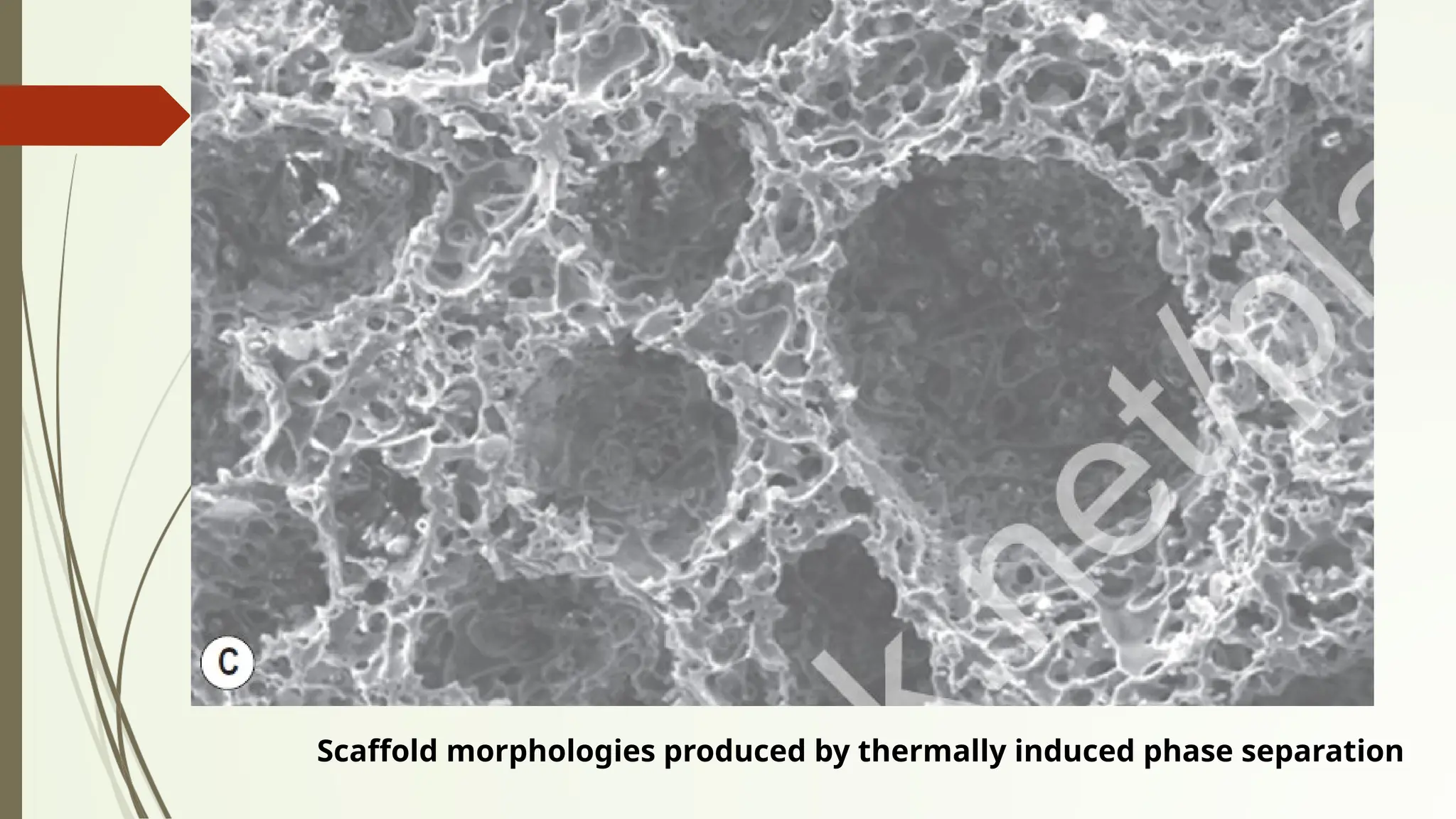
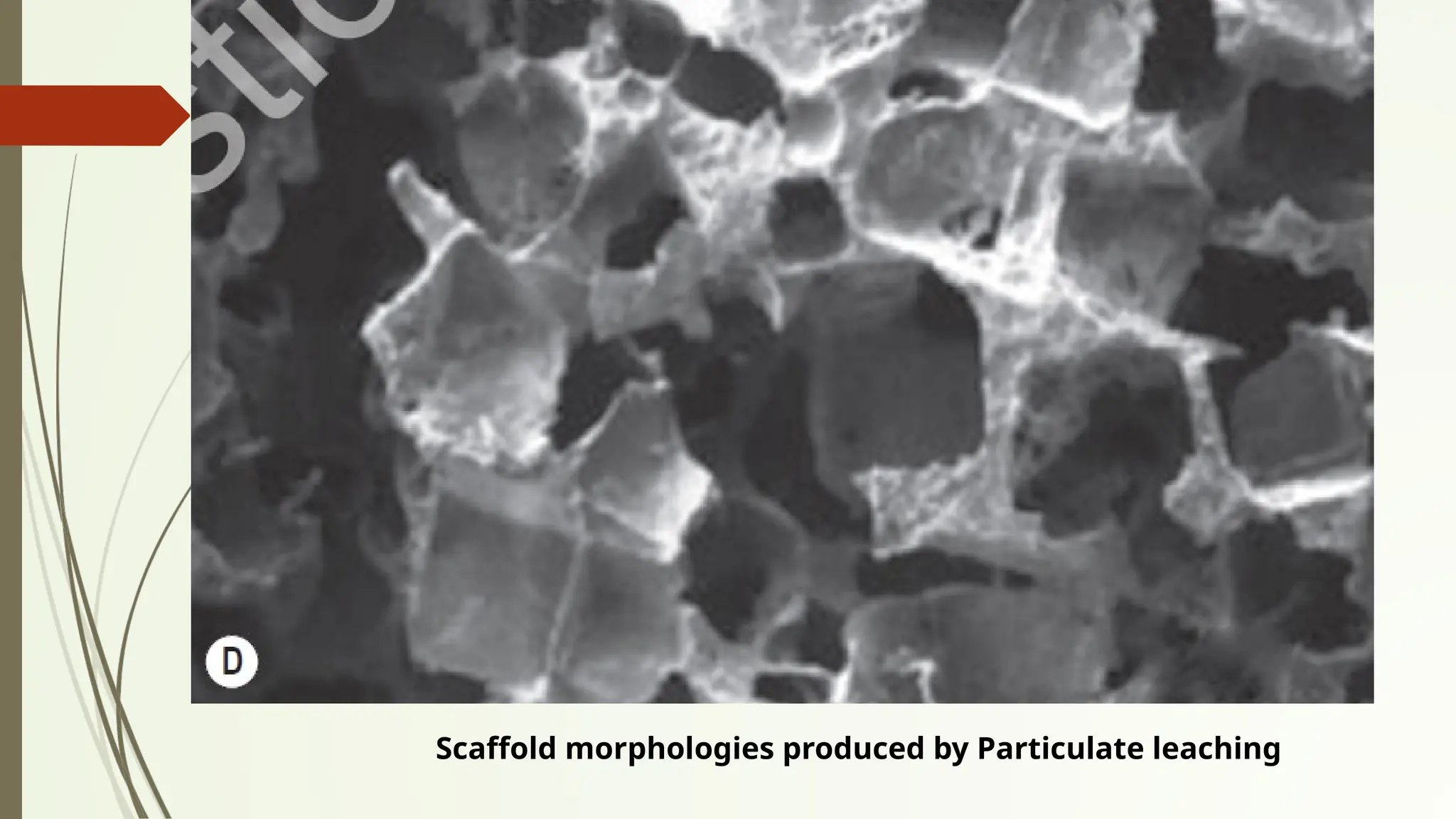
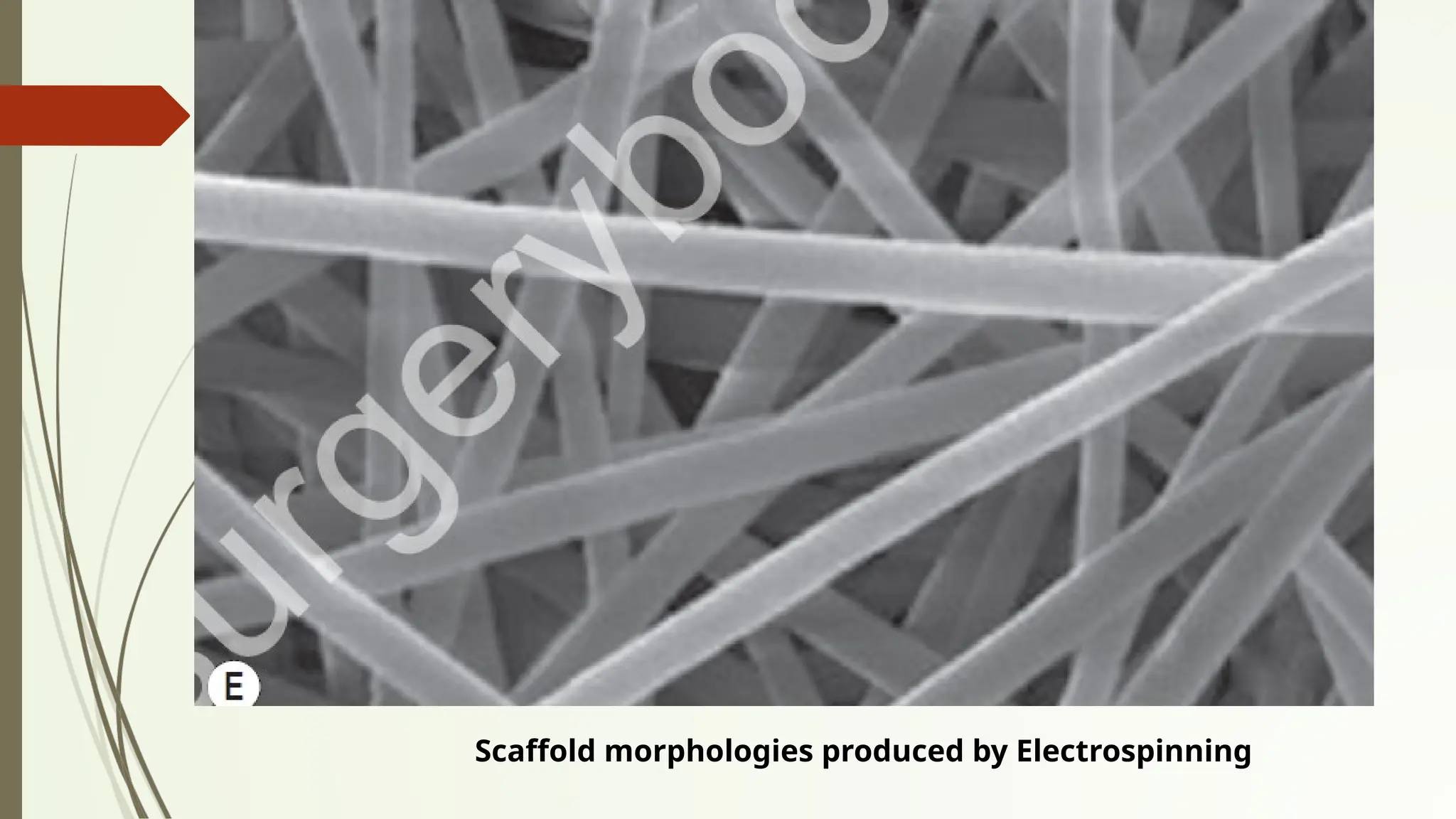
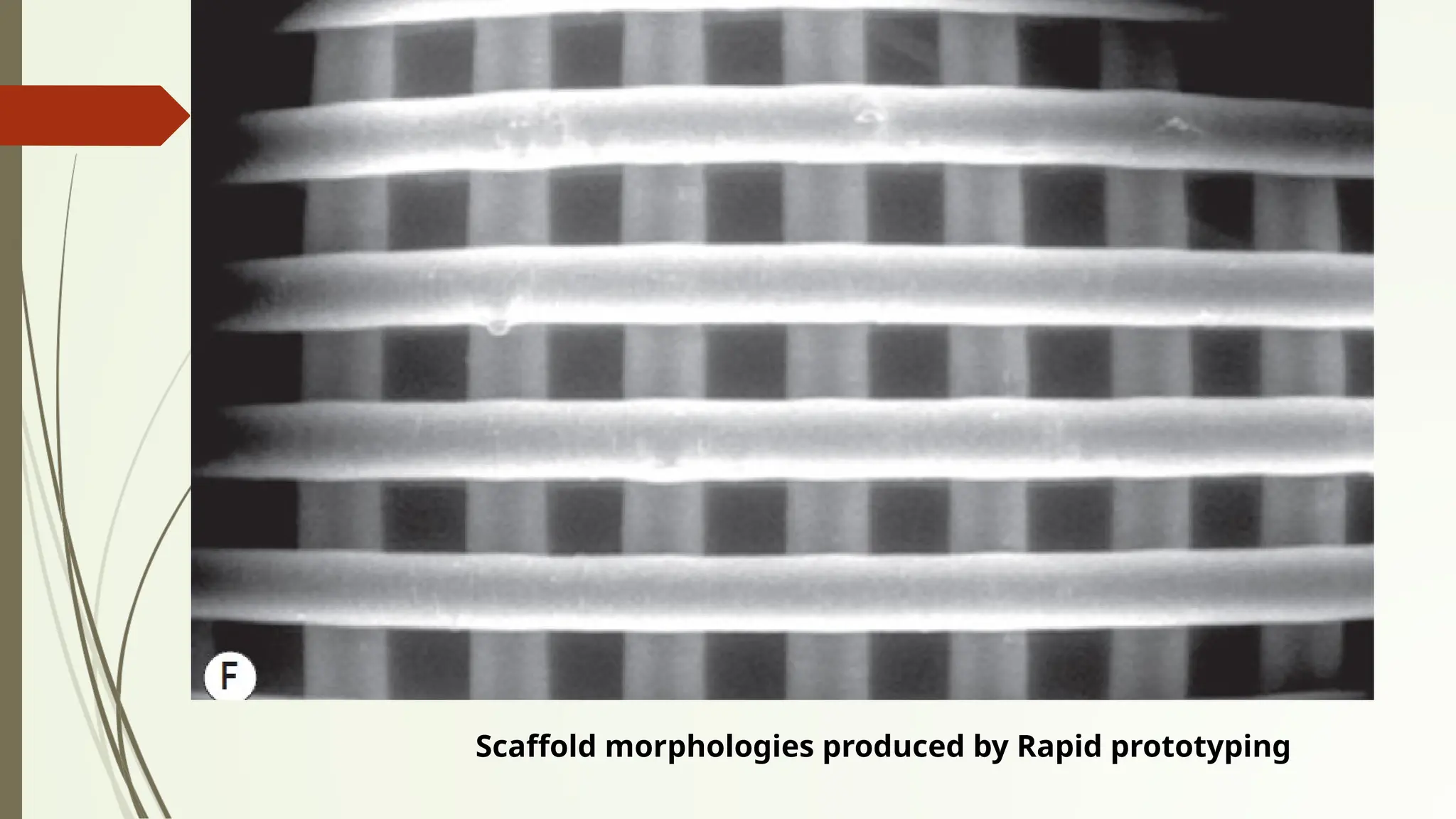
• Techniques
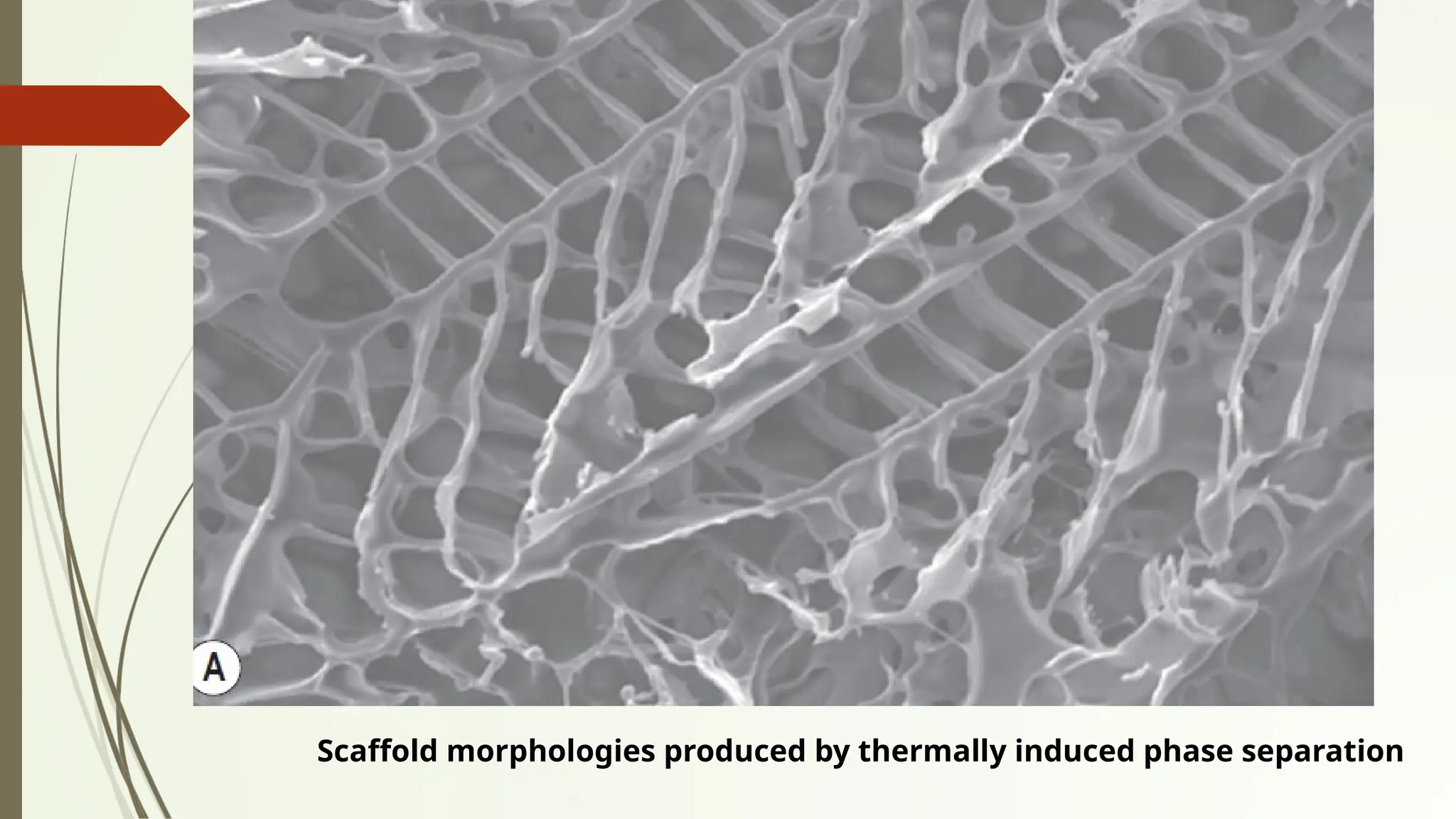
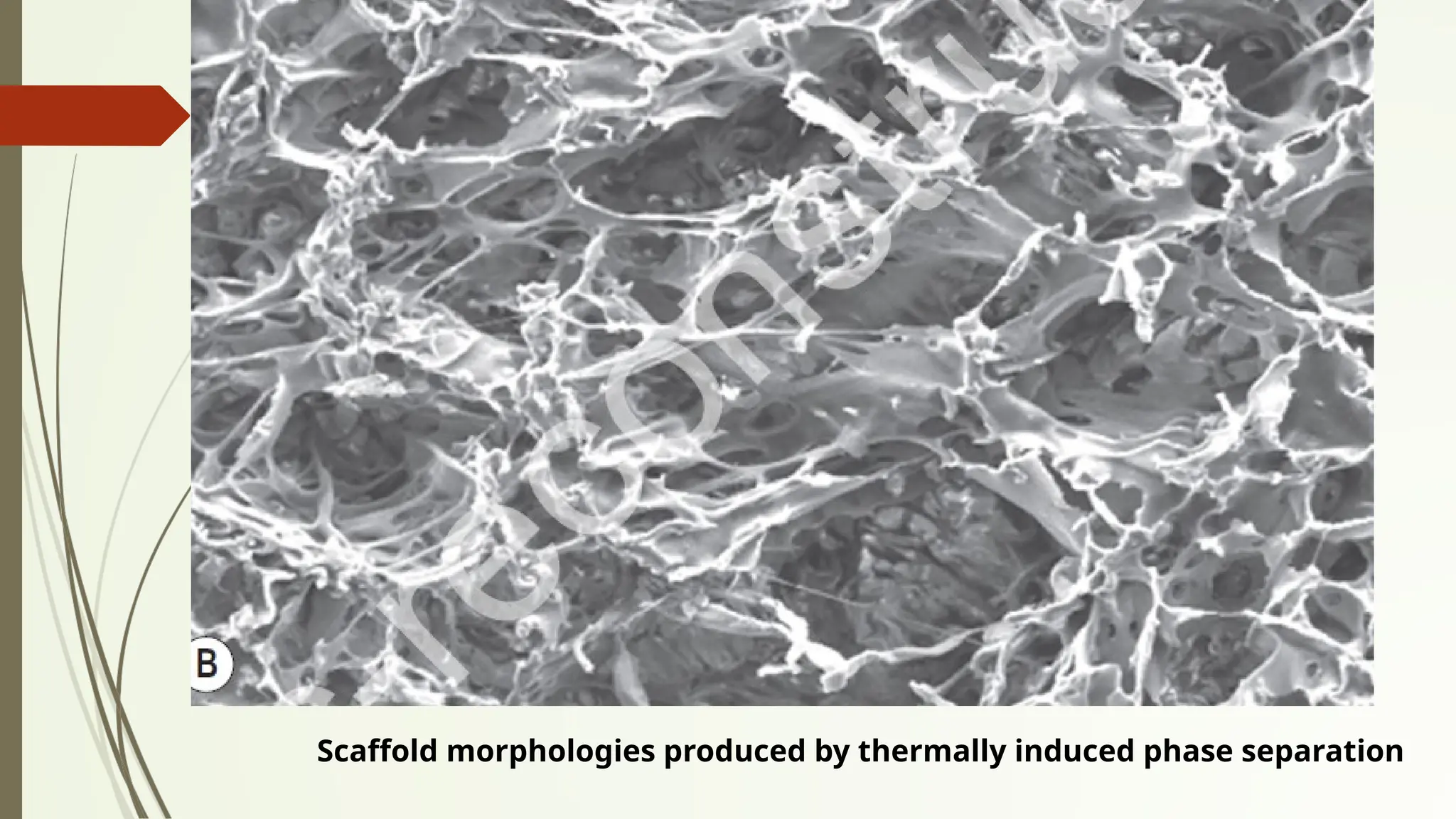
⚬Polymer phase separation
⚬Particle or foam templating
⚬Cryogelation,
⚬Electrospinning
⚬Rapid prototyping methods like 3D-printing.
Scaffolds
• Natural scaffolds
⚬Collagen,Fibrin, Starch, Matrigel ®,Decellularized matrix &
Silk fibrion
• Synthetic materials
⚬Polyethylene glycol, Poly (lactic glycolic) acid and
Polyurethane
• Clinically approved dermal substitutes such as Integra® and
Matriderm ® have also been used for prevascularization
purposes by seeding them with endothelial colony forming
cells (ECFCs) in association with either human dermal
fibroblasts (hDFs) or bone marrow-derived mesenchymal
stem cells (BMSCs).
51.
Growth factors
• VEGF-A- most important in angiogenesis.
⚬Acts mainly by binding to
■ VEGF receptor 1 (VEGFR1) expressed in endothelial cells,
hematopoietic stem cells and inflammatory cells,
■ VEGF receptor 2,(VEGFR2) expressed mainly in endothelial cells.
• FGF-2 (aka basic fibroblast growth factor, bFGF)
• Mostly involved in angiogenesis
• Produced by a number of differentiated cells e.g.
keratinocytes, mast cells, fibroblasts, endothelial cells and
smooth muscle cells, as well as by adult mesenchymal stem
cells derived from bone marrow, adipose, and dermal
tissue.
52.
Growth factors
• FGF-2- Stimulating migration and proliferation of
endothelial cells in vivo,
• Mitogenesis of smooth muscle cells and fibroblasts, which
induces the development of large collateral vessels with
adventitia.
• FGF-2 - In the prevascularization of scaffolds - Faster
inosculation of the scaffold in vivo
• PDGF-B released by endothelial cells - Angiogenesis process
mainly by attracting pericytes that will subsequently
provide stability and structural support to the newly formed
vessel.