Thyroiditis refers to inflammation of the thyroid gland and can be caused by various factors such as viruses, bacteria, fungi, autoimmune disorders and medications. The document discusses the different types of thyroiditis including acute infectious, subacute, Riedel's, postpartum, autoimmune and amiodarone-induced thyroiditis. It provides details on symptoms, diagnostic testing, treatment and prognosis for each type. Genetic and environmental risk factors for developing autoimmune thyroid disease are also reviewed.
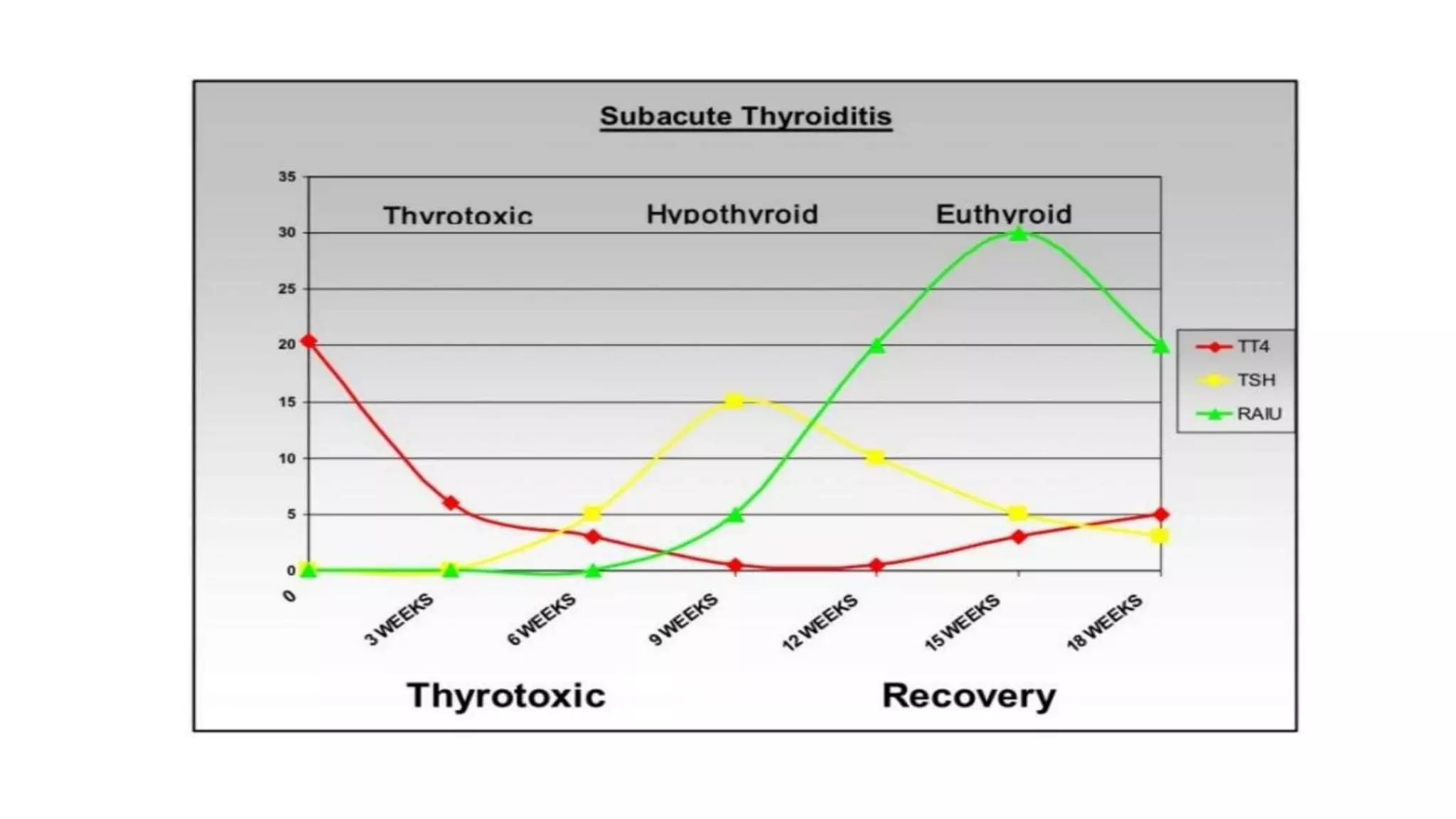
![• Painless (silent, autoimmune) subacute thyroiditis occurs spontaneously or following pregnancy when it is
referred to as postpartum thyroiditis [PPT]).
• Autoimmune thyroiditis is histologically similar to Hashimoto's thyroiditis and occurs following 3.9-10% of
pregnancies.
• The combination of thyroid enlargement usually without discomfort and positive anti-thyroid antibodies
associated with typical thyroid function test abnormalities over a 9-12 month course - PLSAT.](https://image.slidesharecdn.com/thyroiditis-230828141311-fccb77be/75/Thyroiditis-pptx-10-2048.jpg)

![• AITD is a component of some rare monogenic syndromes. Autoimmune hypothyroidism affects patient with type 1
polyendocrinopathy; immune dysregulation, 'polyendocrinopathy' and enteropathy [IPEX].
• Different alleles of MHC class I molecule - Graves' disease- HLA-A10, B8 and DQw2 is seen in India.
• Cytotoxic T lymphocyte antigen-4 (CTLA-4) -an immunomodulatory molecule expressed on the surface of activated T cell,
is its key negative regulator.
• CTLA-4 gene is a major candidate gene for common autoimmune disorders like Graves' disease, Type-1 diabetes and
Hashimoto's thyroiditis.](https://image.slidesharecdn.com/thyroiditis-230828141311-fccb77be/75/Thyroiditis-pptx-38-2048.jpg)