Downloaded 110 times

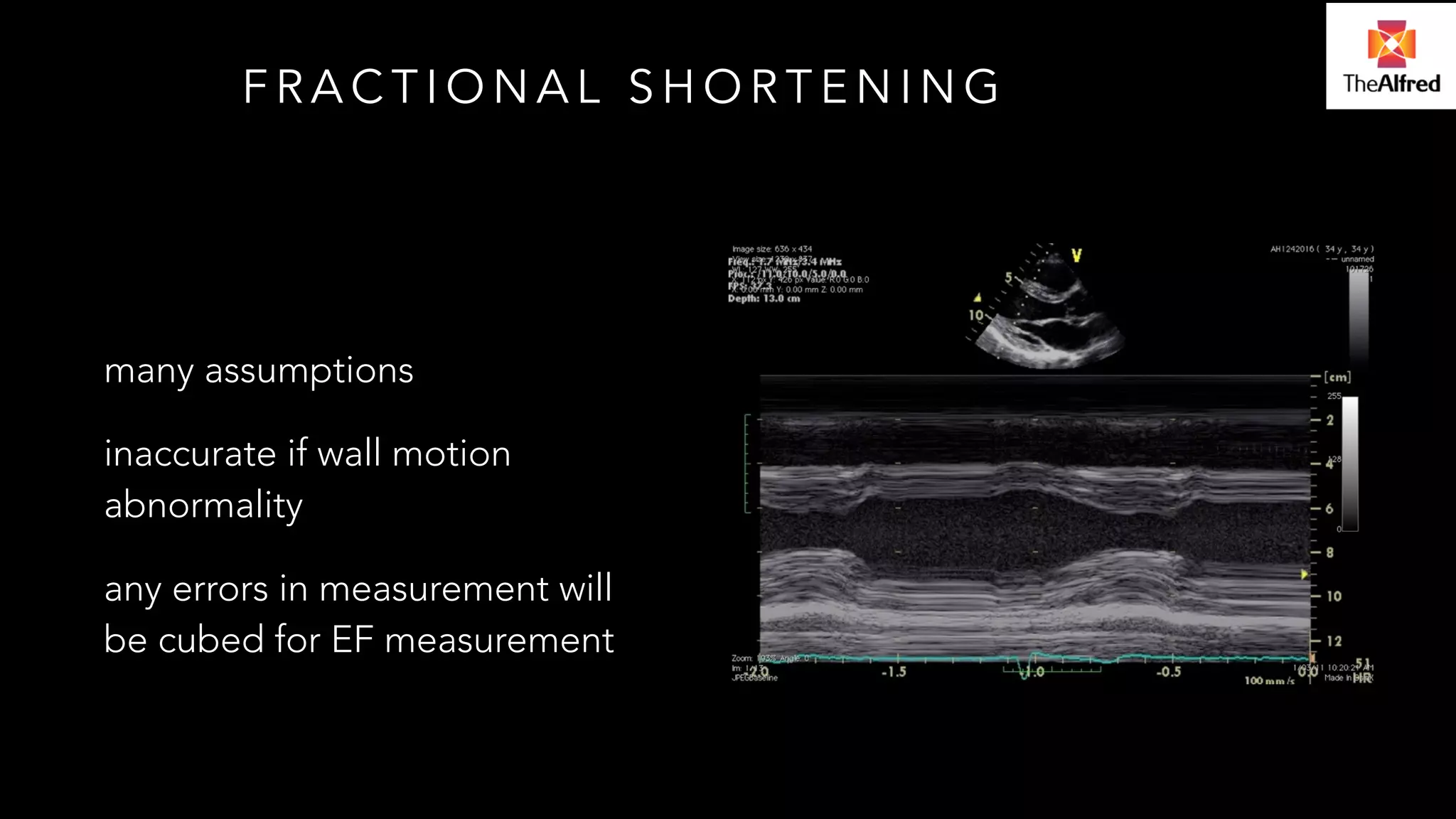

The document discusses the role of echocardiography (echo) in assessing hemodynamics and the complexities of using echocardiographic measurements in critically ill patients. It highlights the assumptions and limitations of different echocardiographic methods, emphasizing the importance of accurate measurement techniques to avoid errors in cardiac function assessments. Additionally, it covers various parameters used to evaluate fluid responsiveness and the impact of interventions in specific clinical scenarios.
Introduction to Deirdre Murphy Alfred ICU, discussing the truth and assumptions regarding echocardiography.
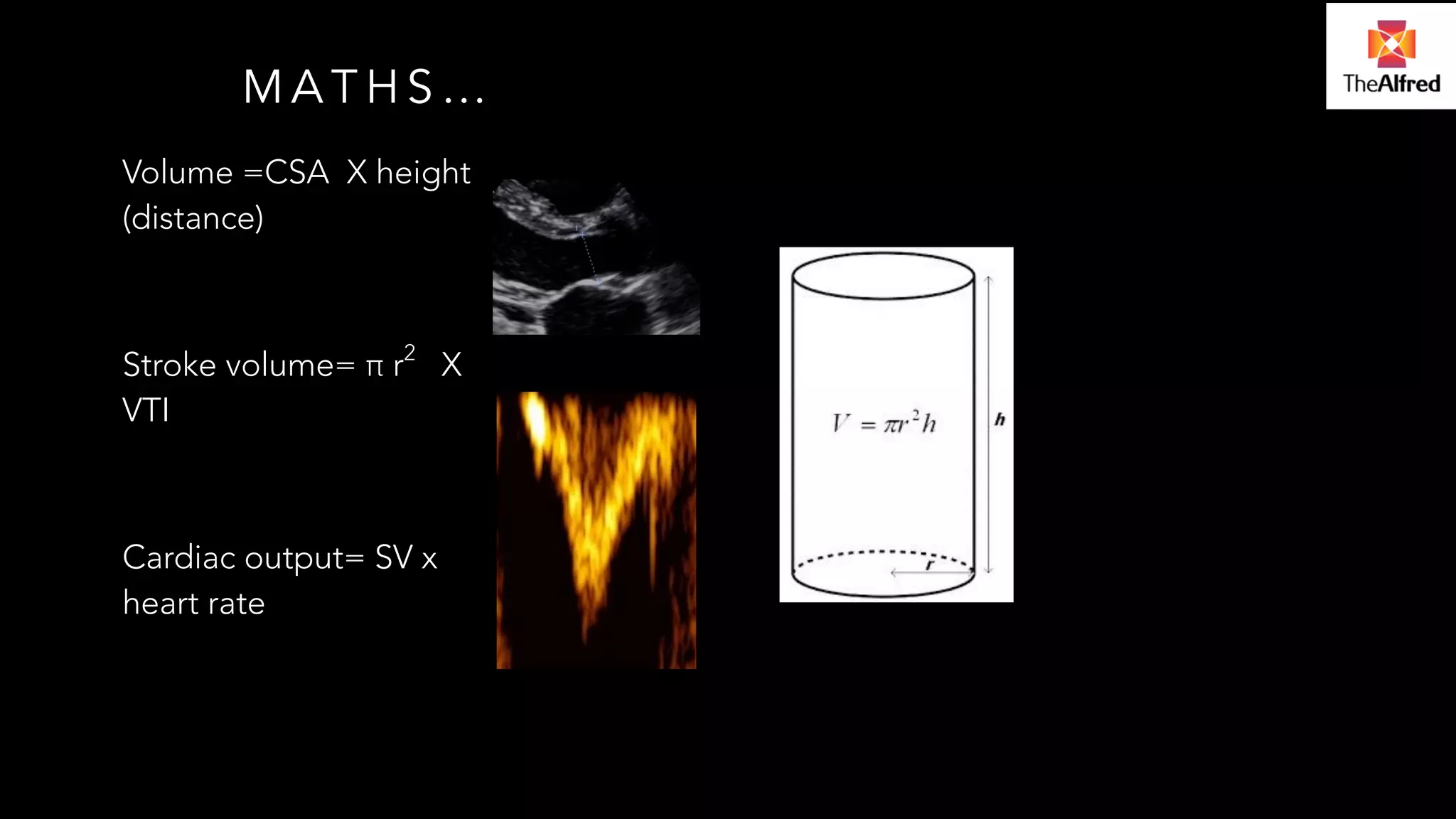
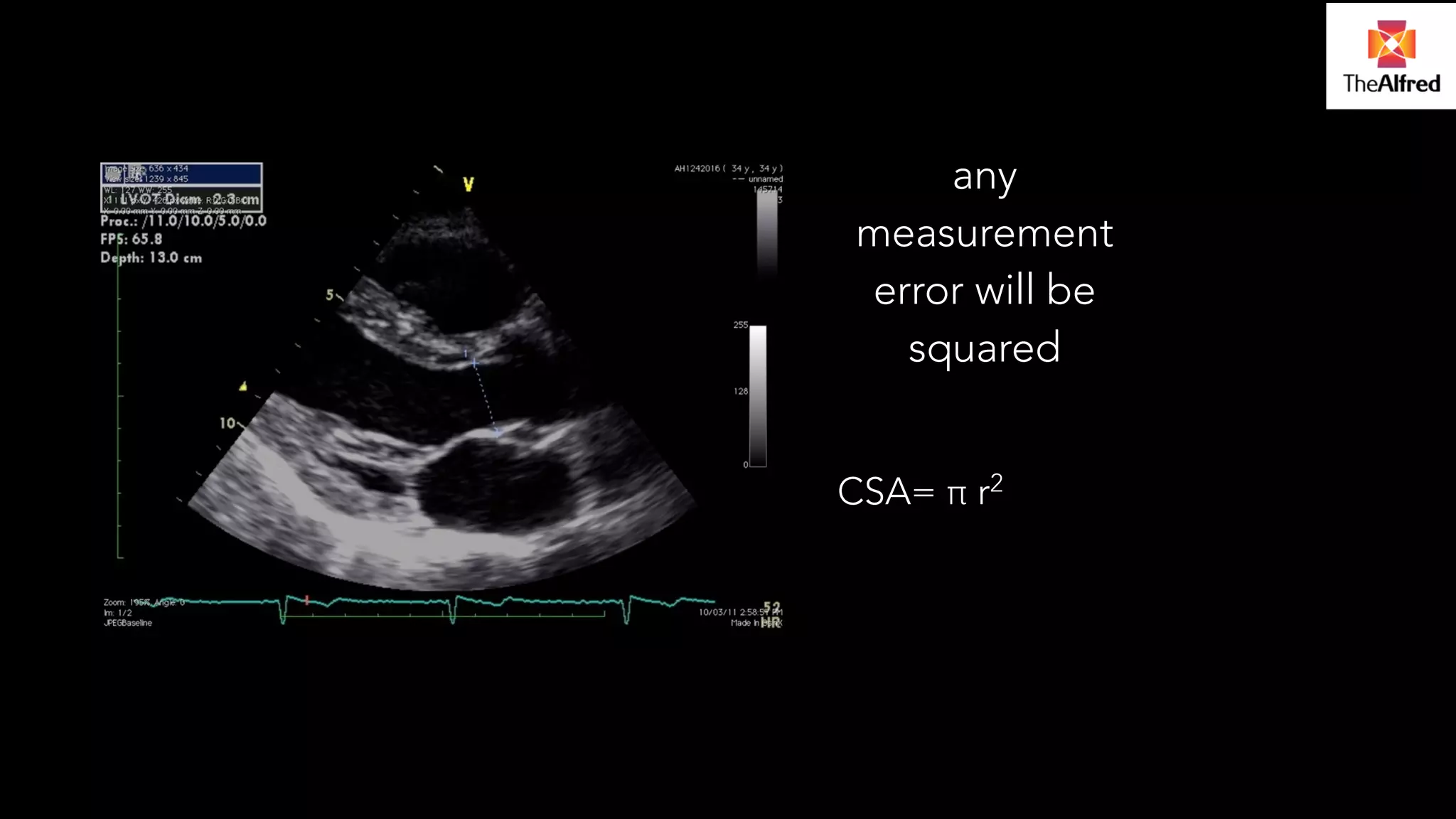
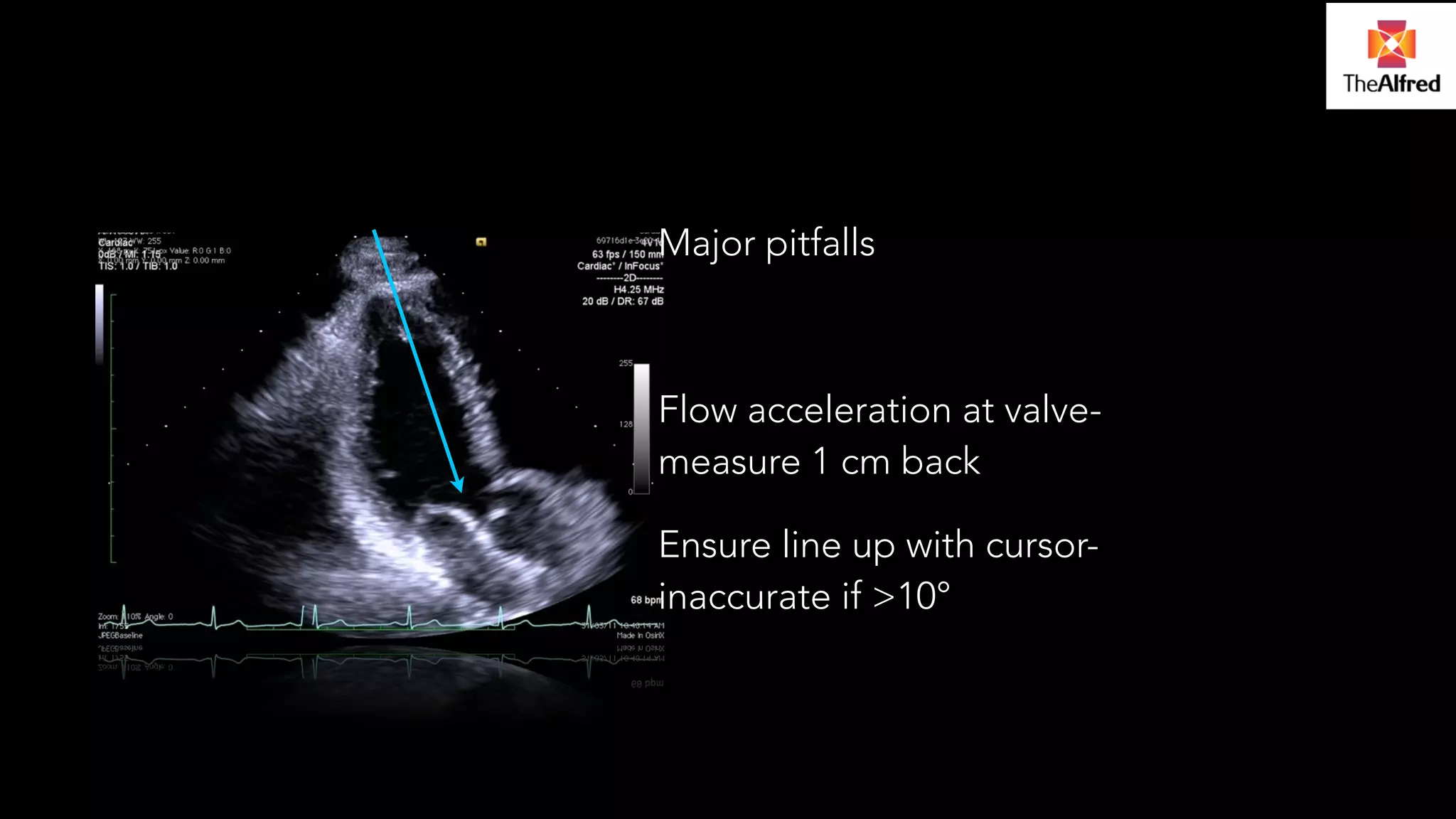
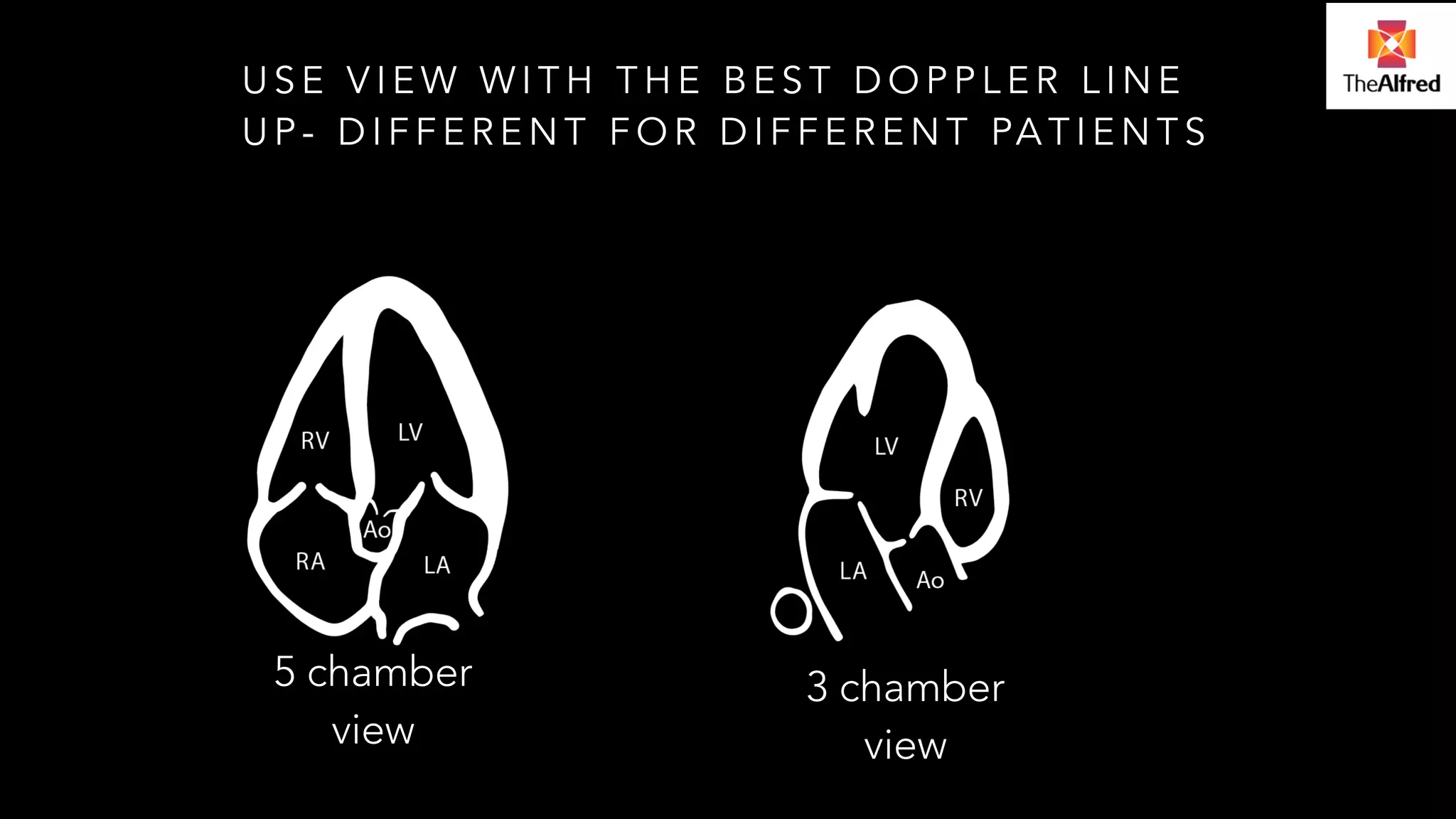
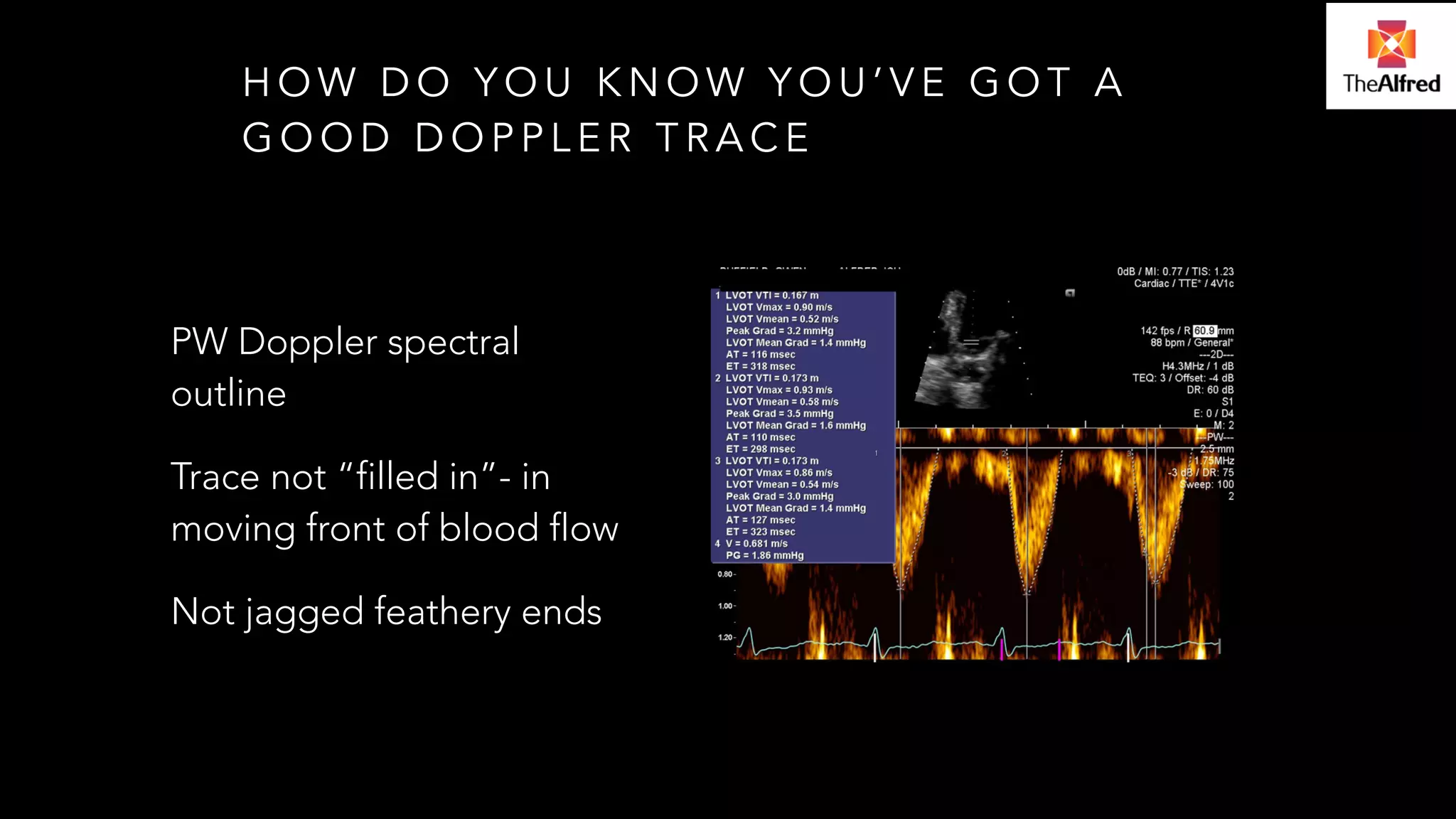
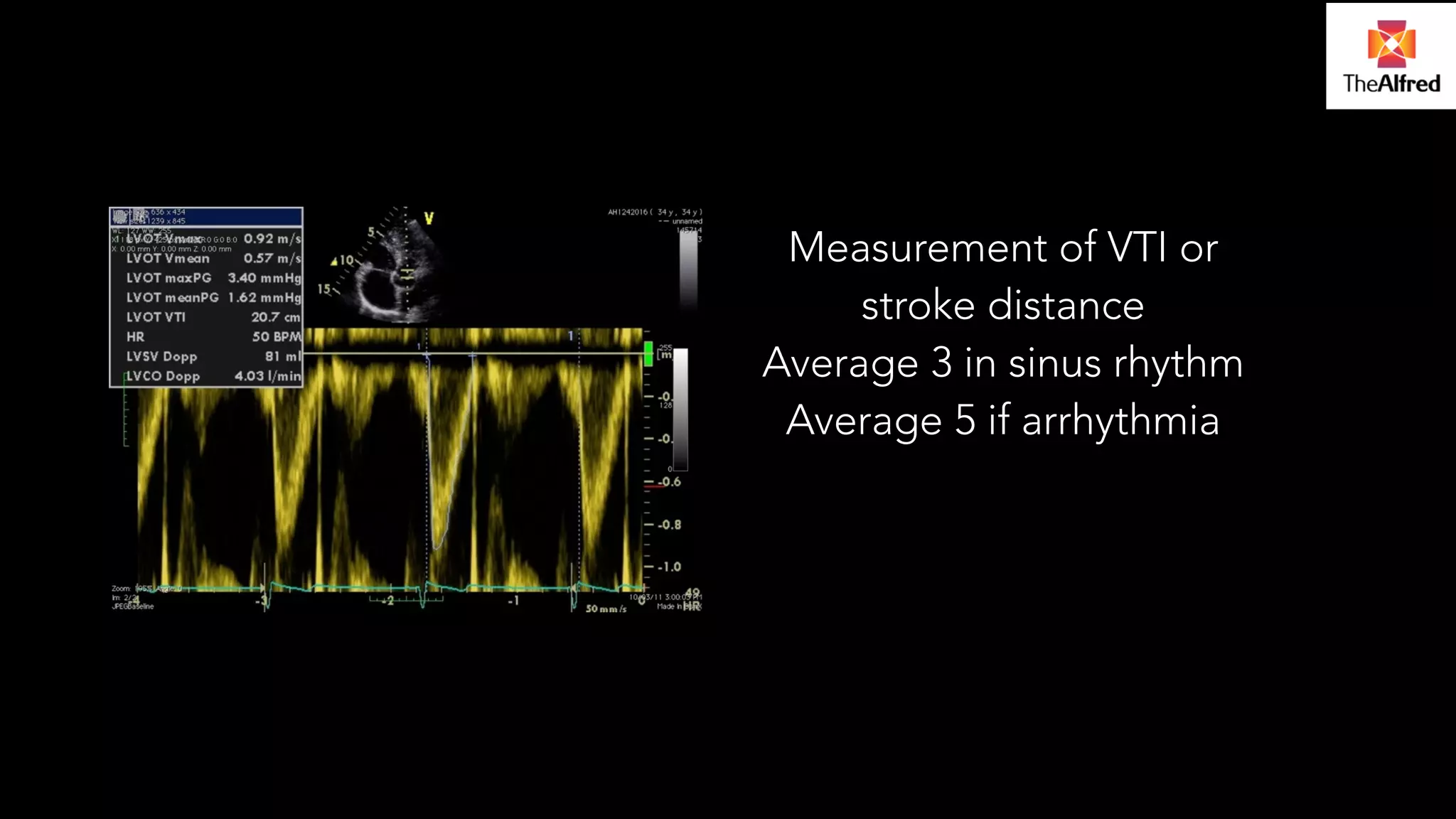
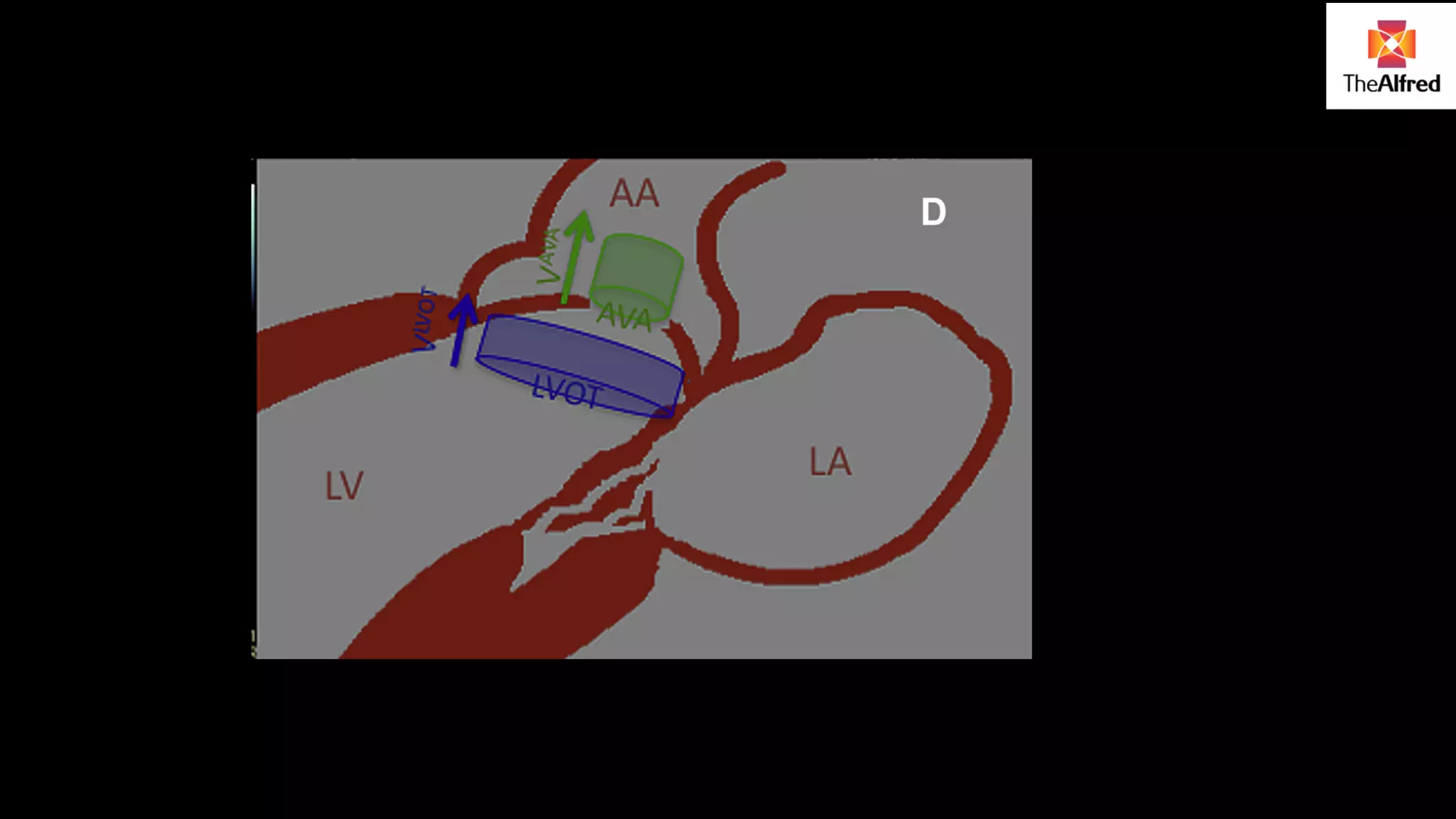
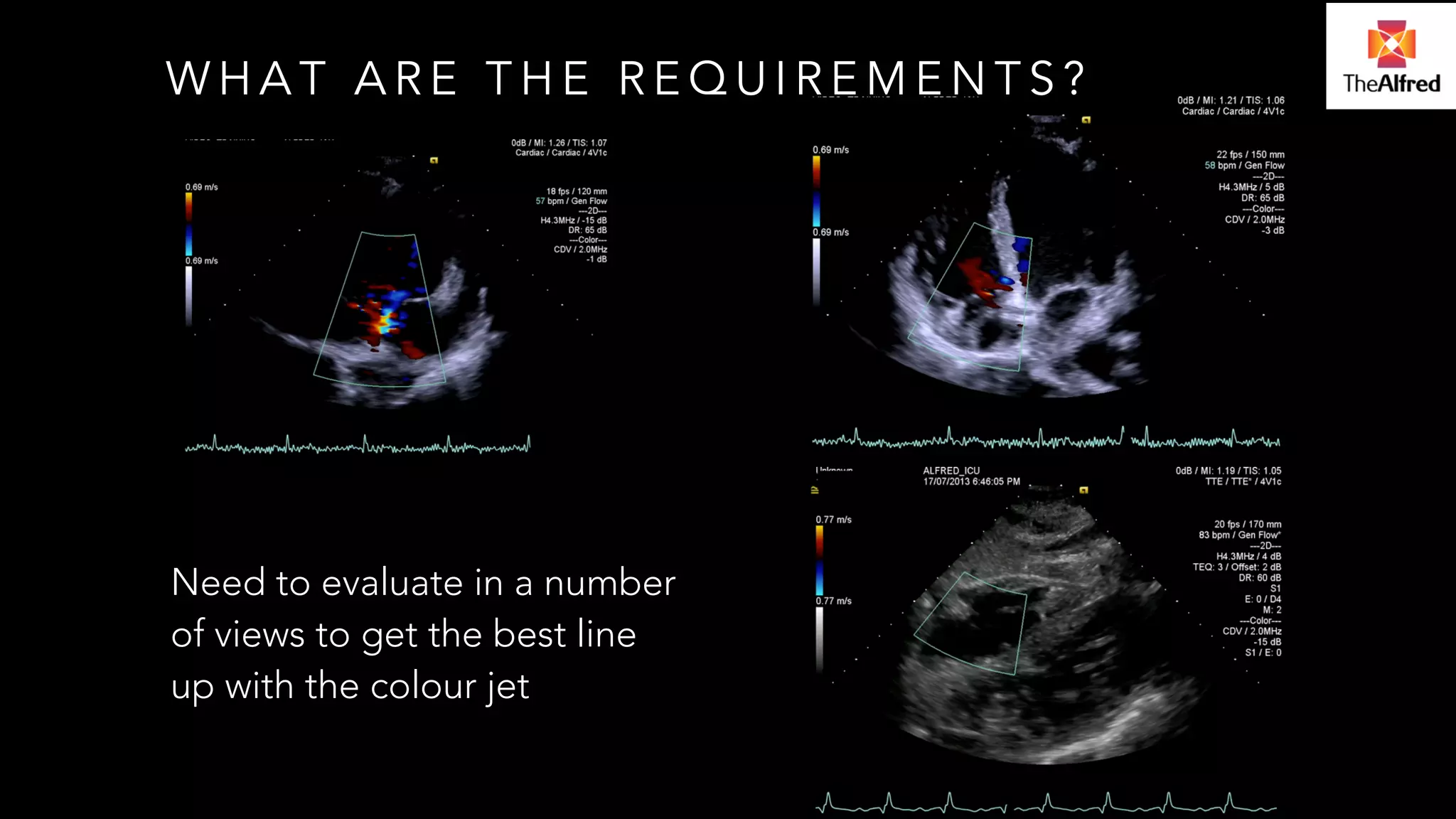
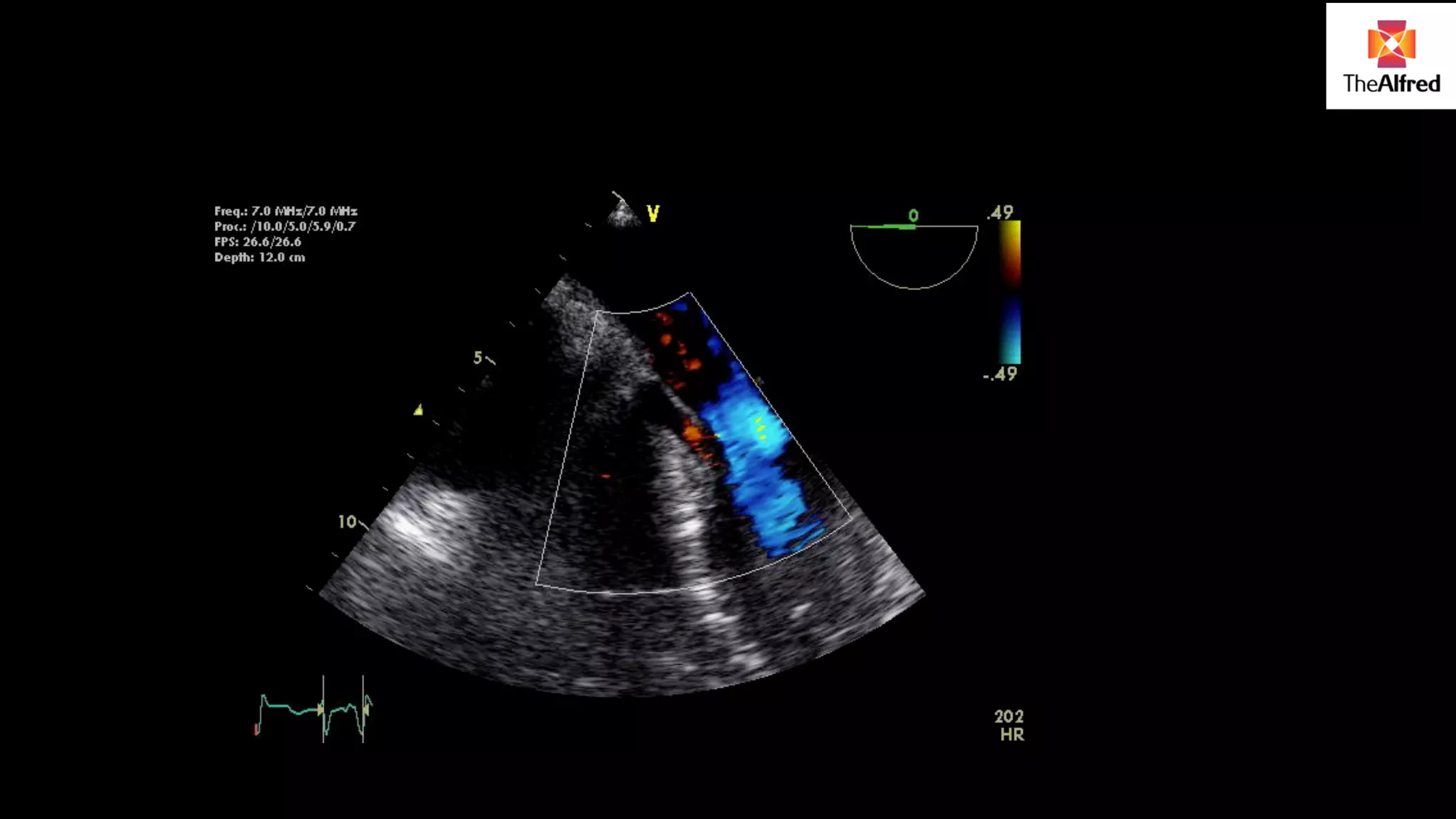
Emphasizes understanding limitations and methodologies in echographic assessments, including common hemodynamic information. Discusses achieving good Doppler traces, understanding flow patterns, and maintaining accurate measurements through various views.
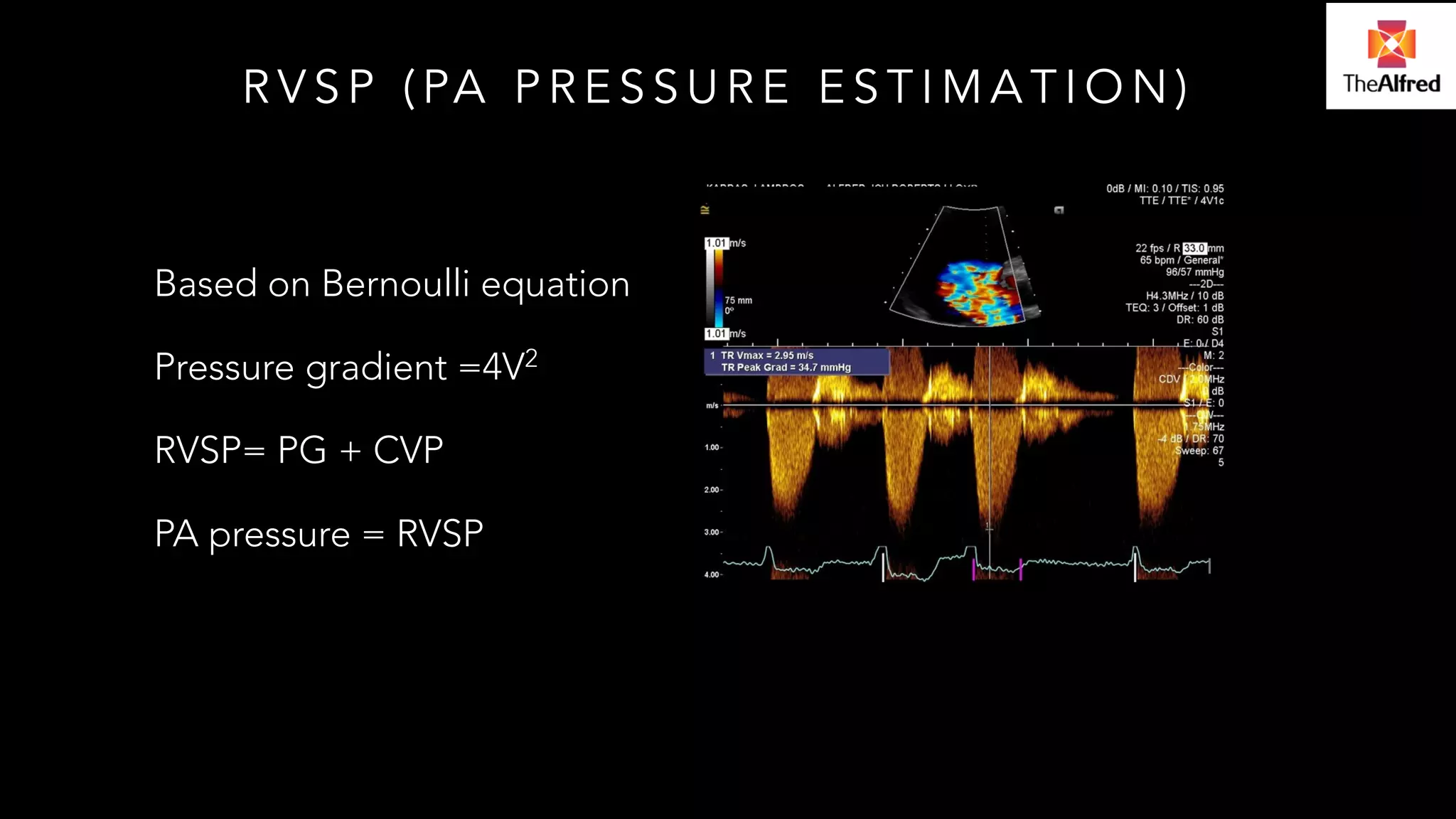
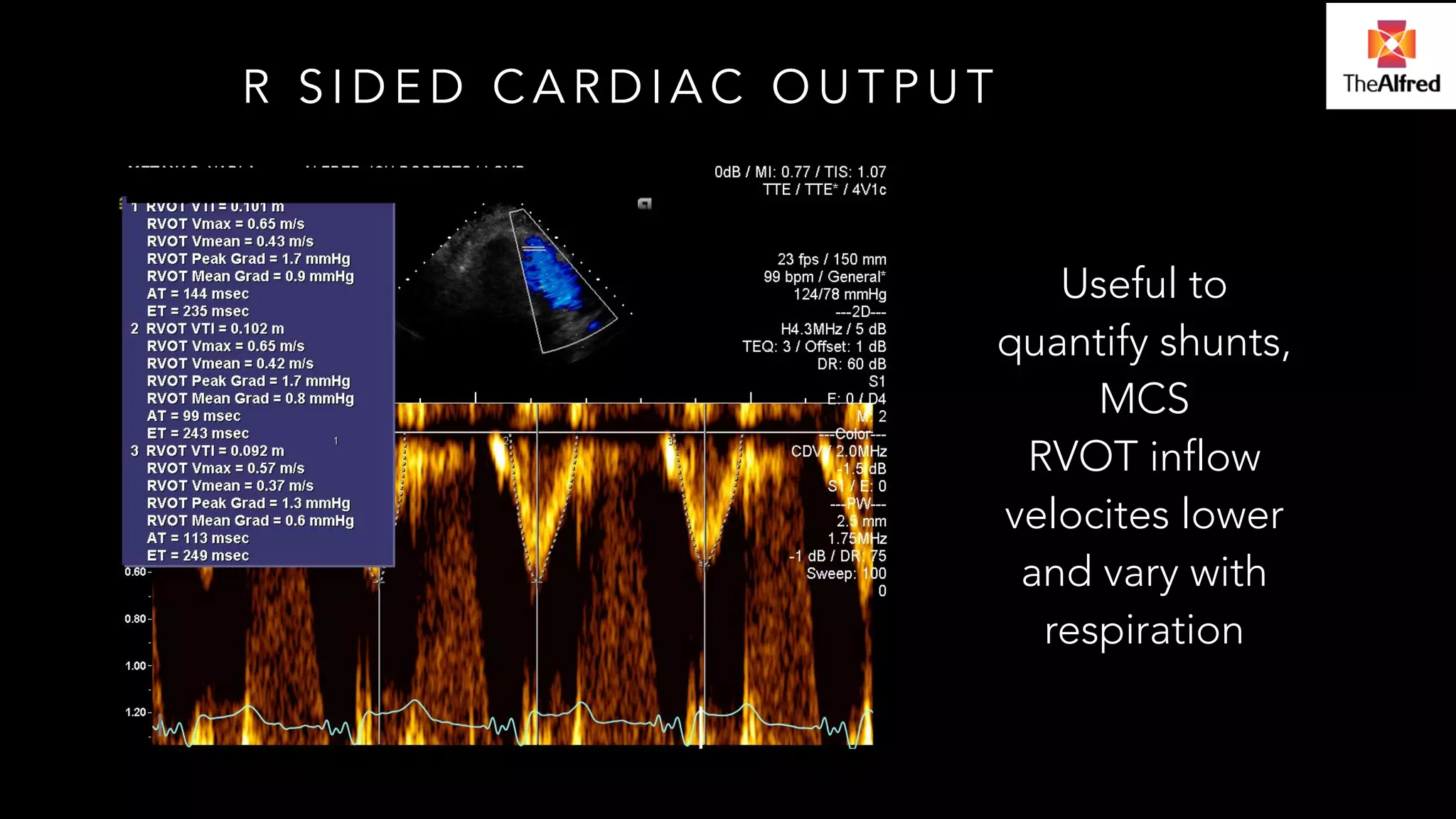
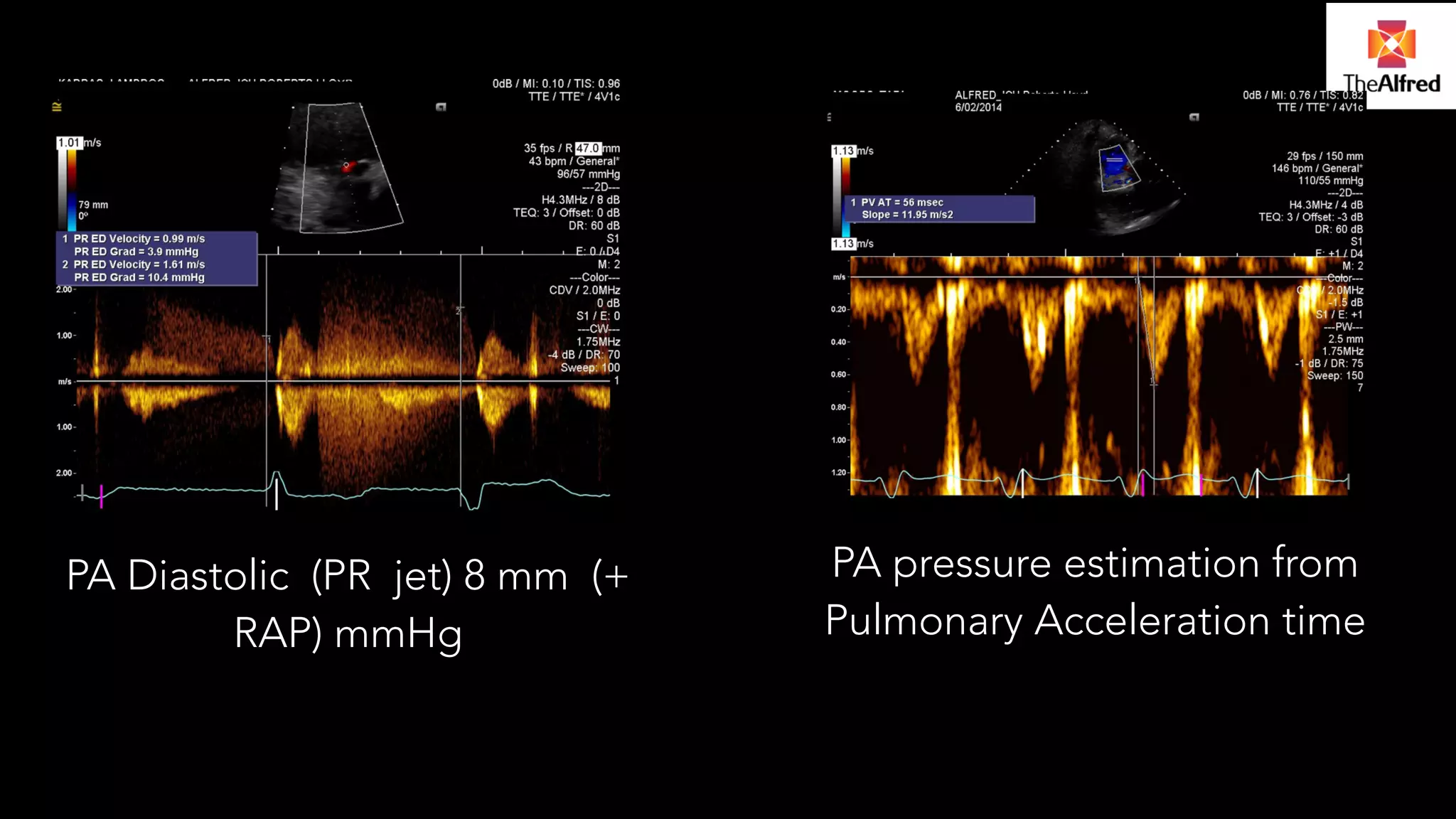
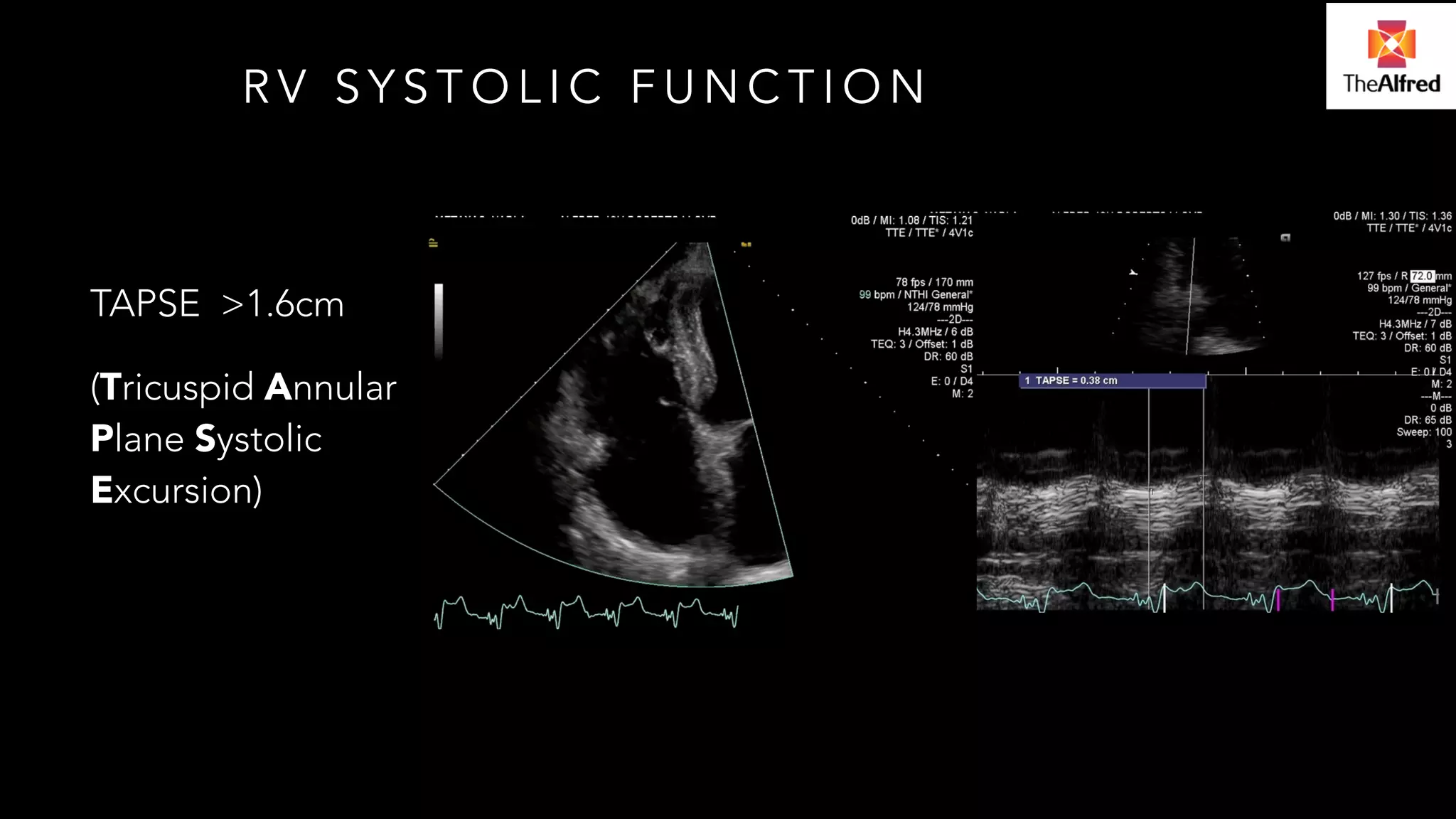
Explores the evaluation of right-sided cardiac output and pulmonary acceleration time for PA pressure estimation.
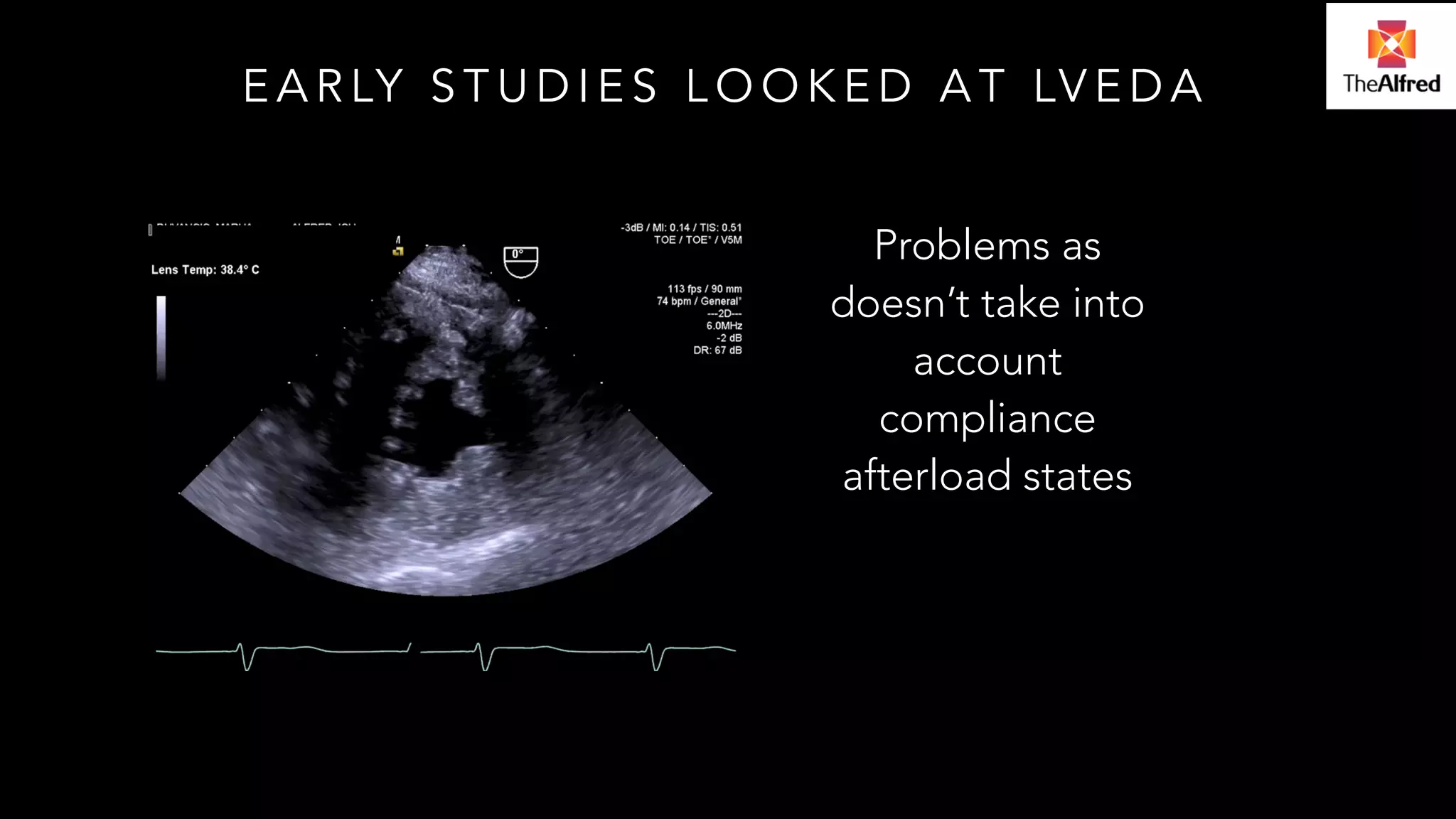
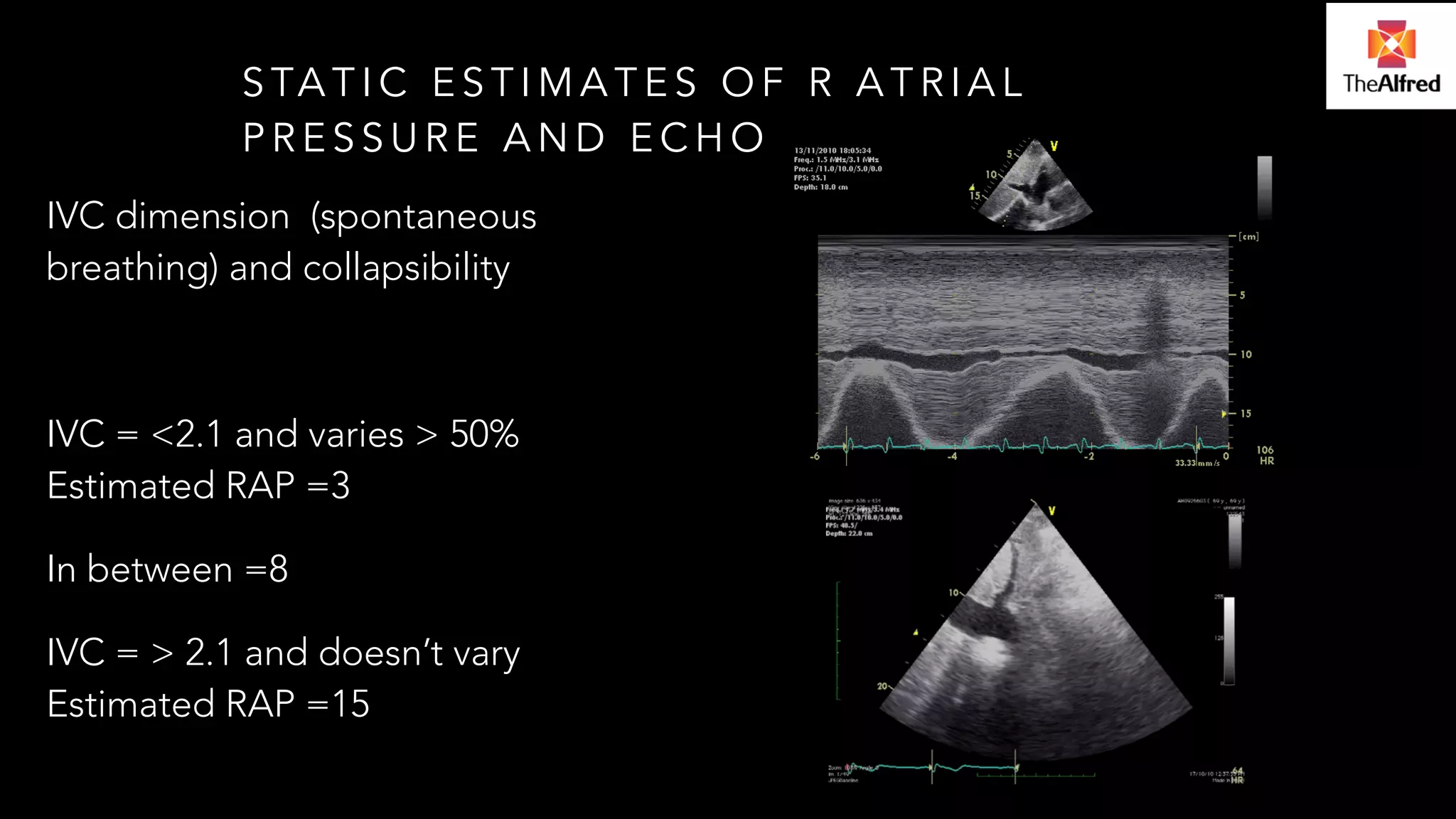
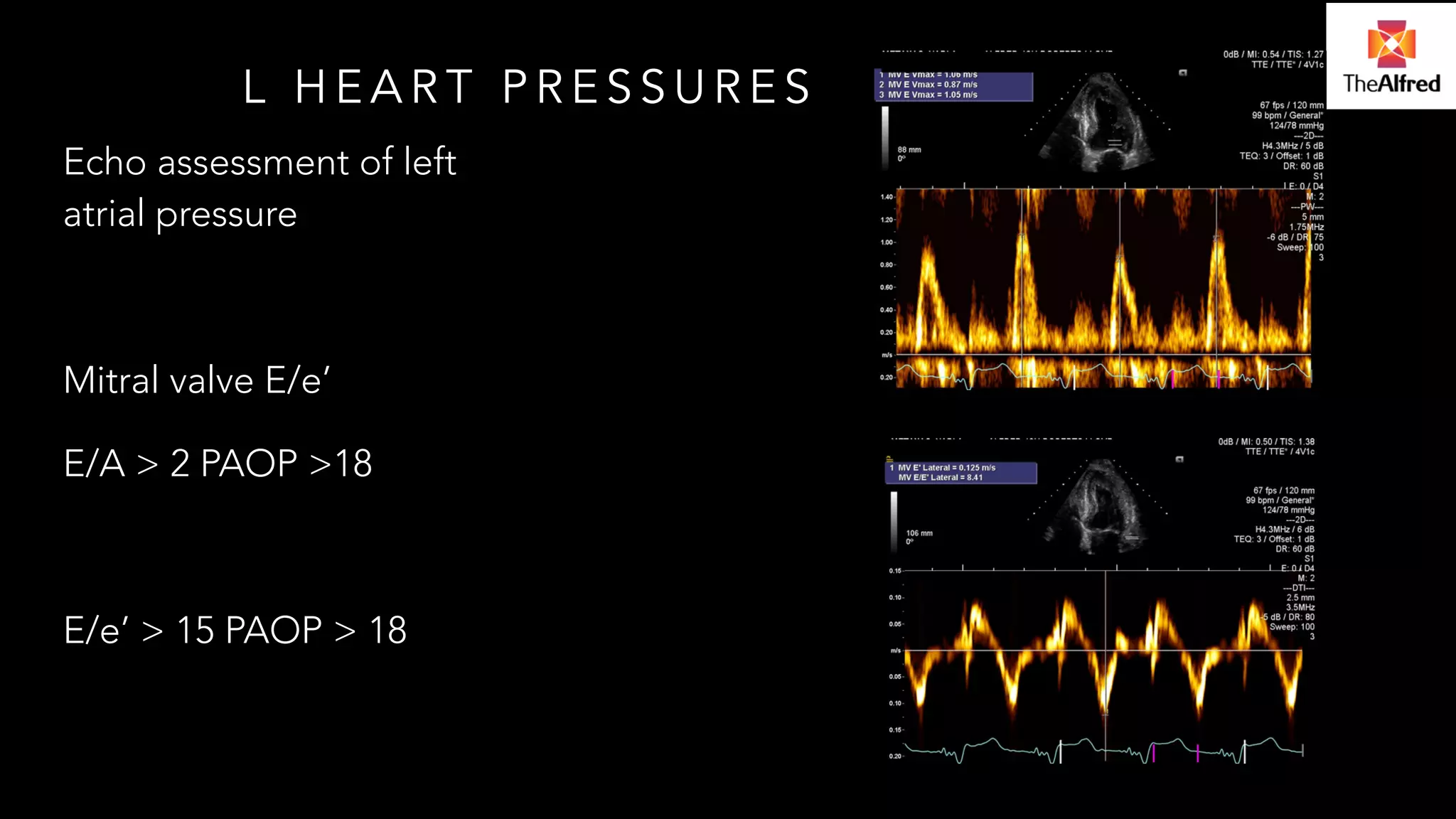
Investigates early studies on left atrial pressure estimates from IVC dimensions, important for assessing volume states.
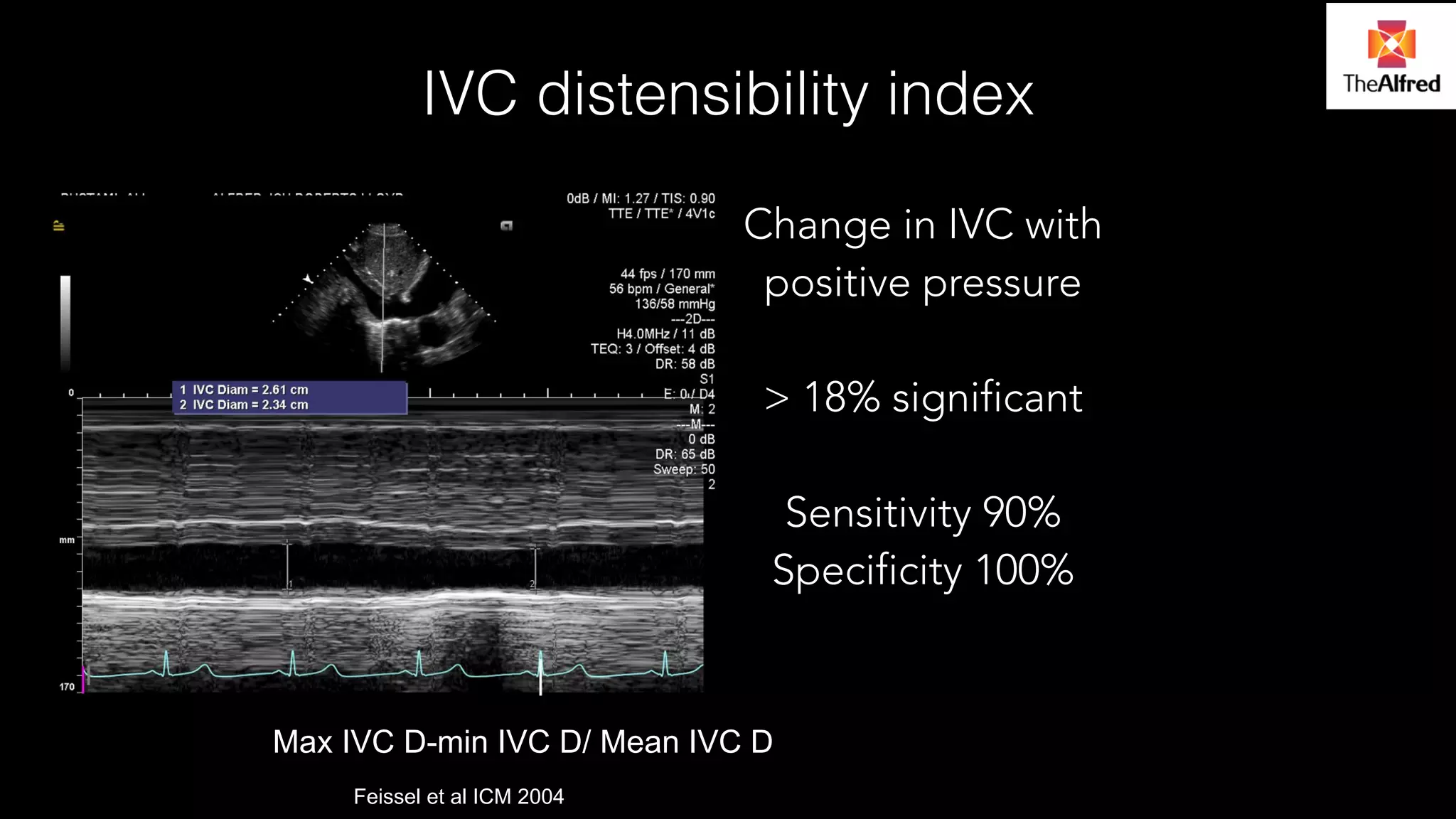
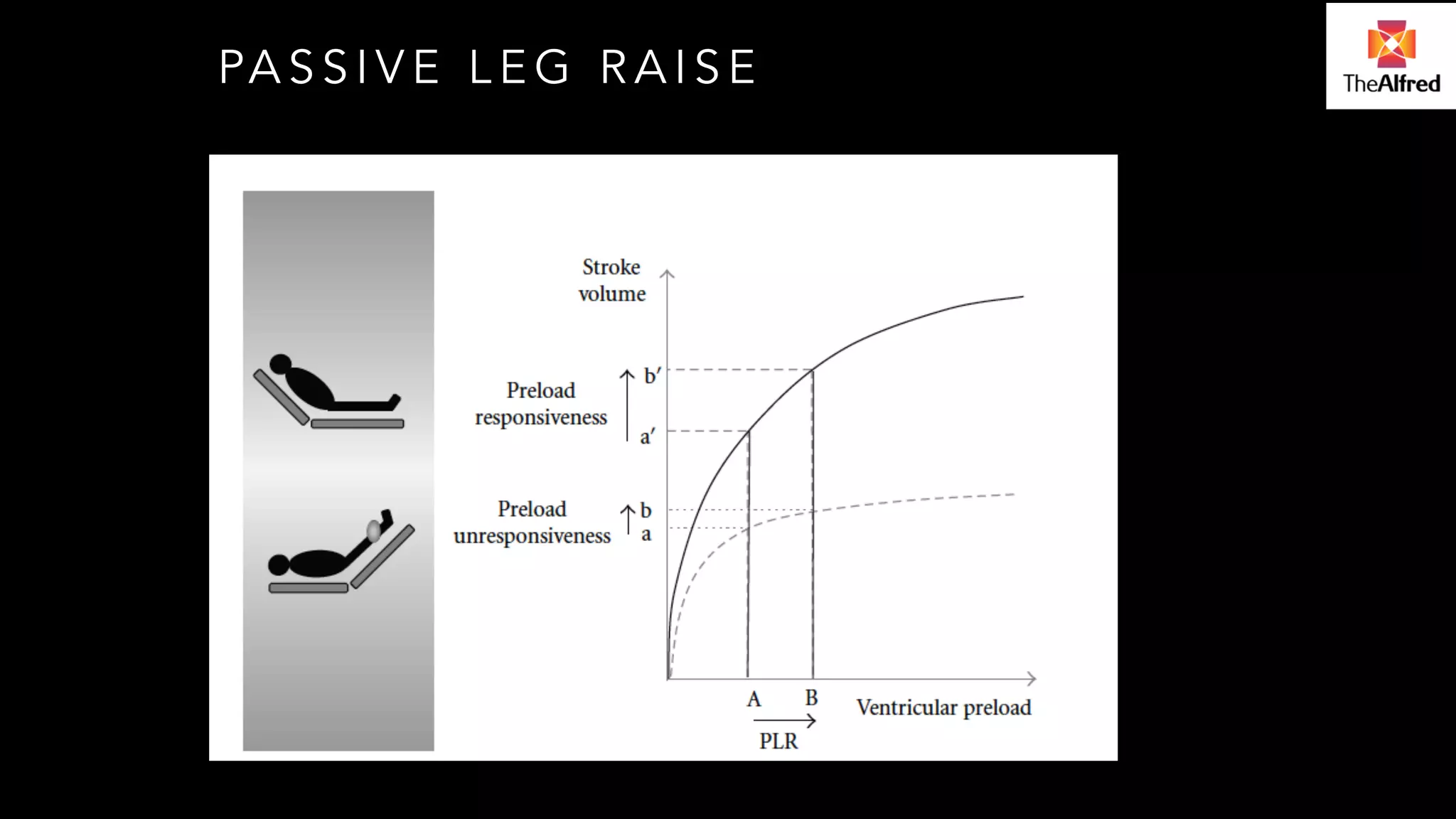
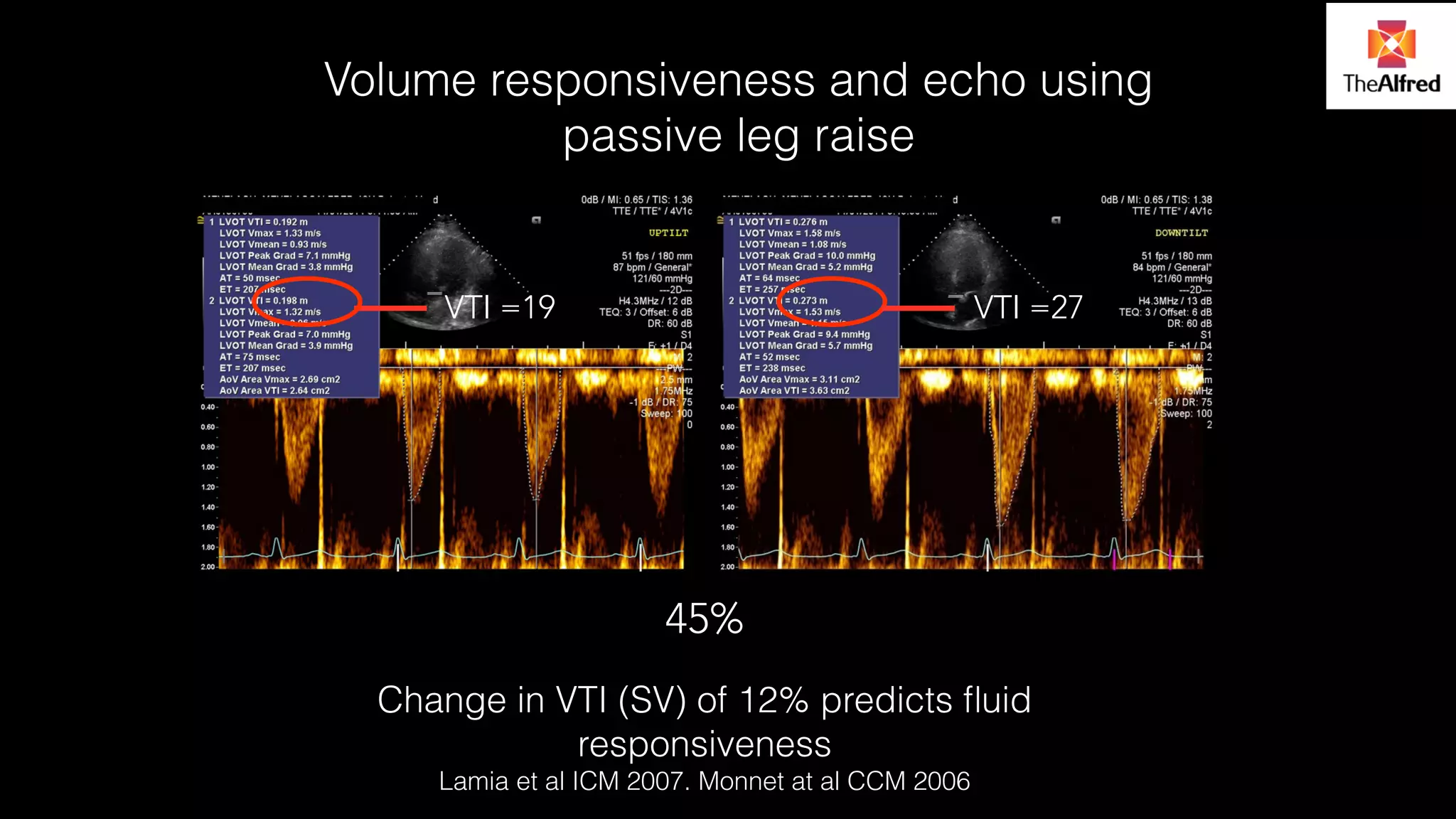
Functional evaluation of hemodyanamics, including IVC distensibility index and the predictive value of passive leg raises.
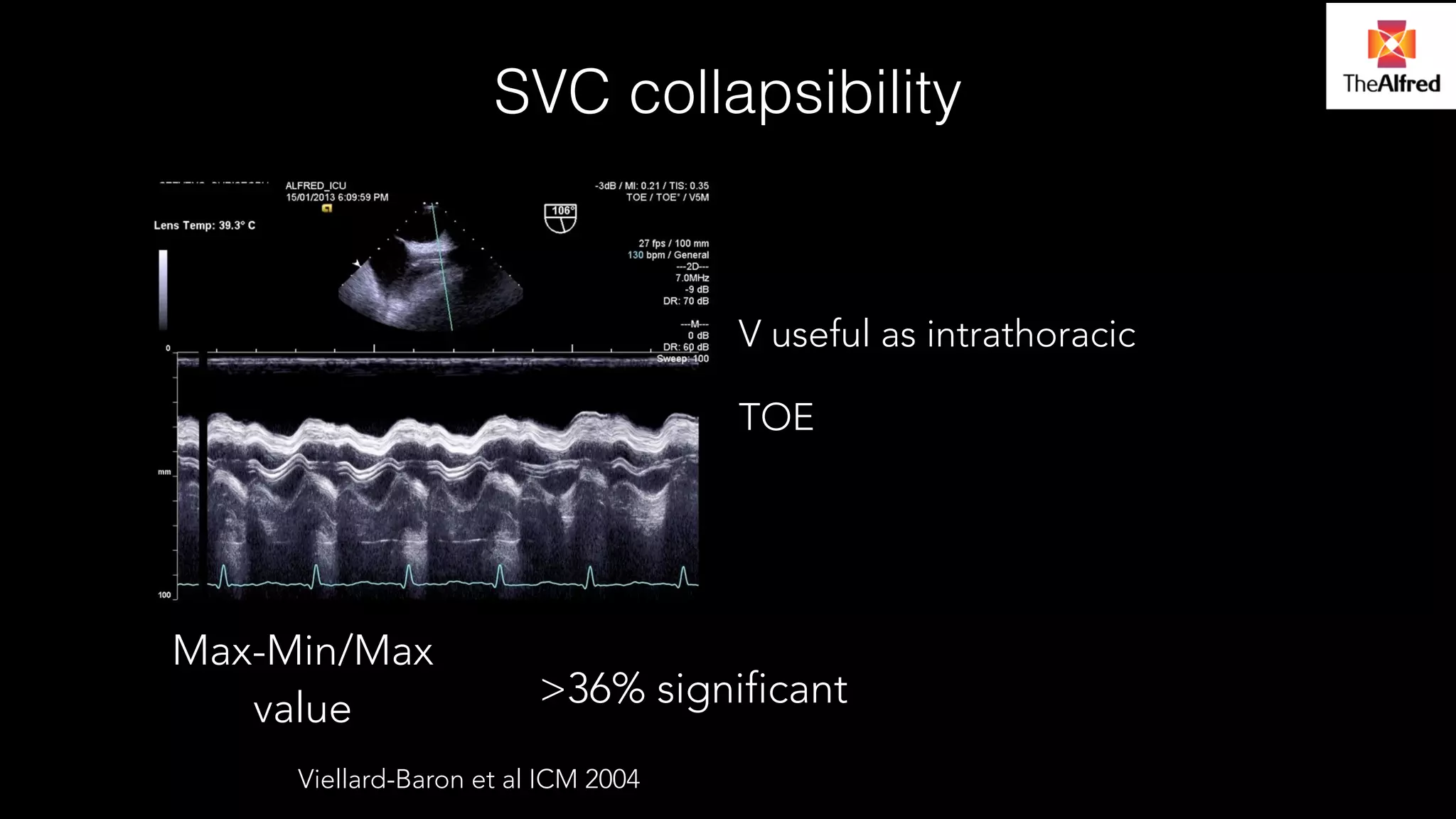
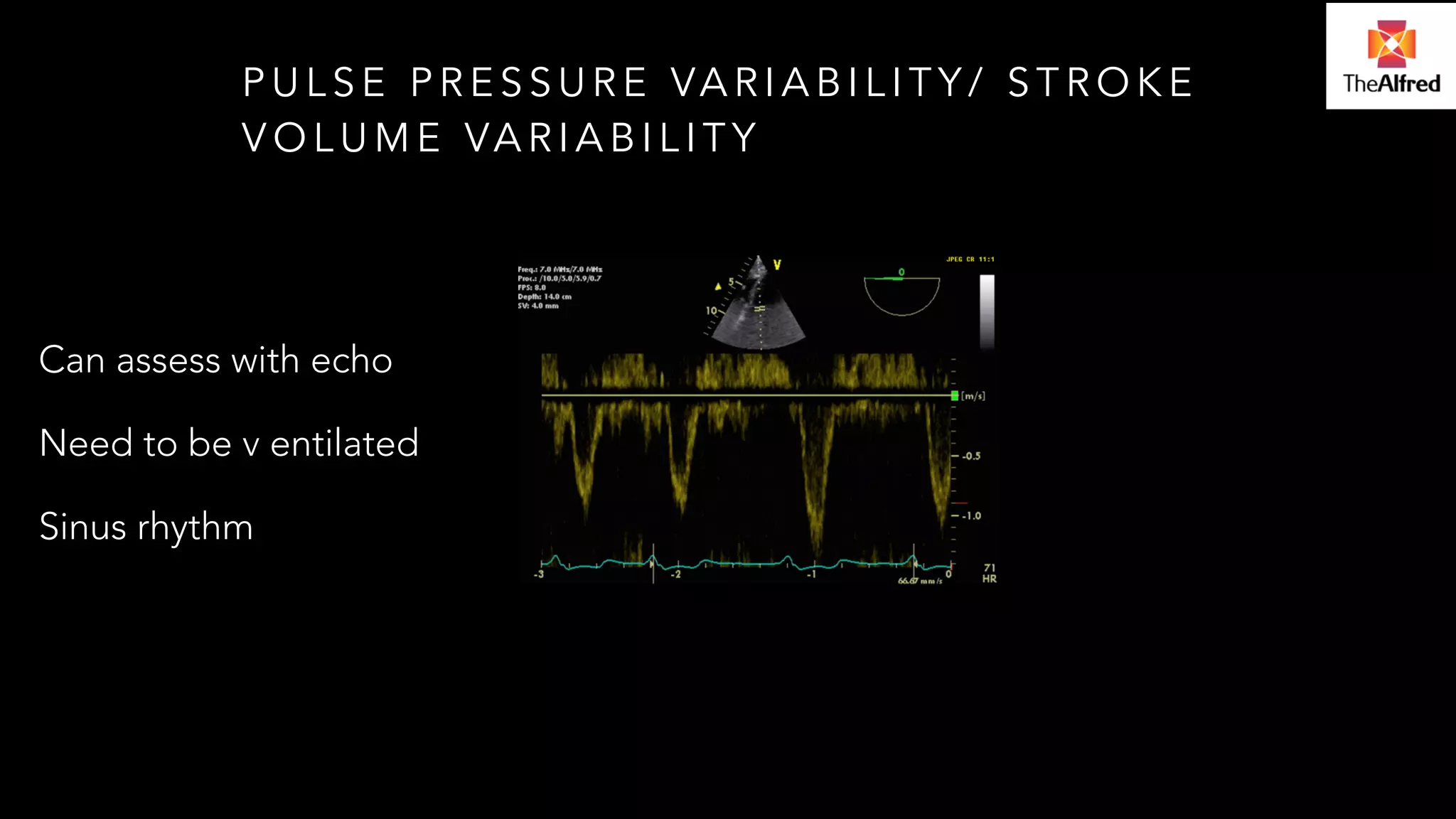
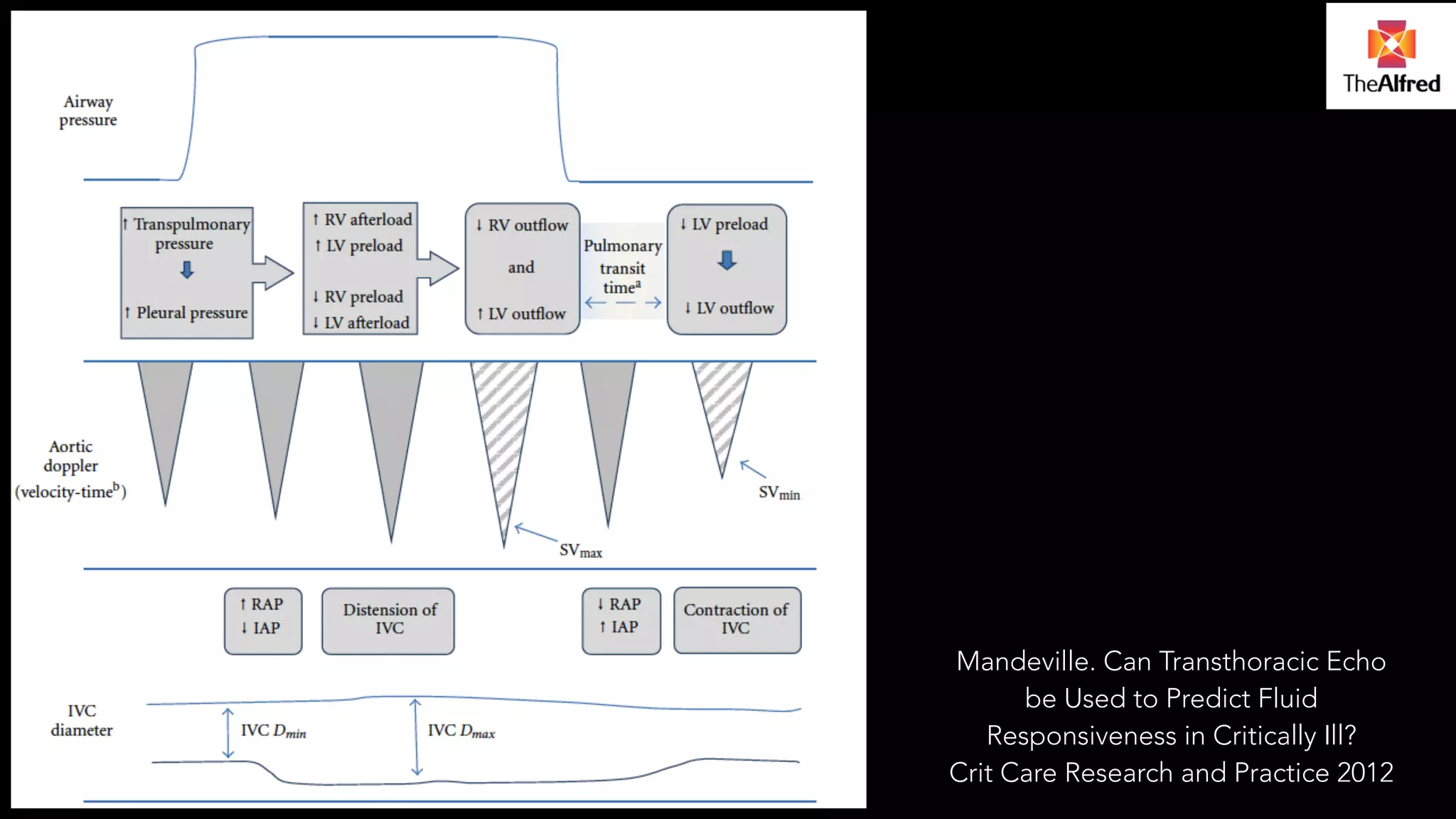
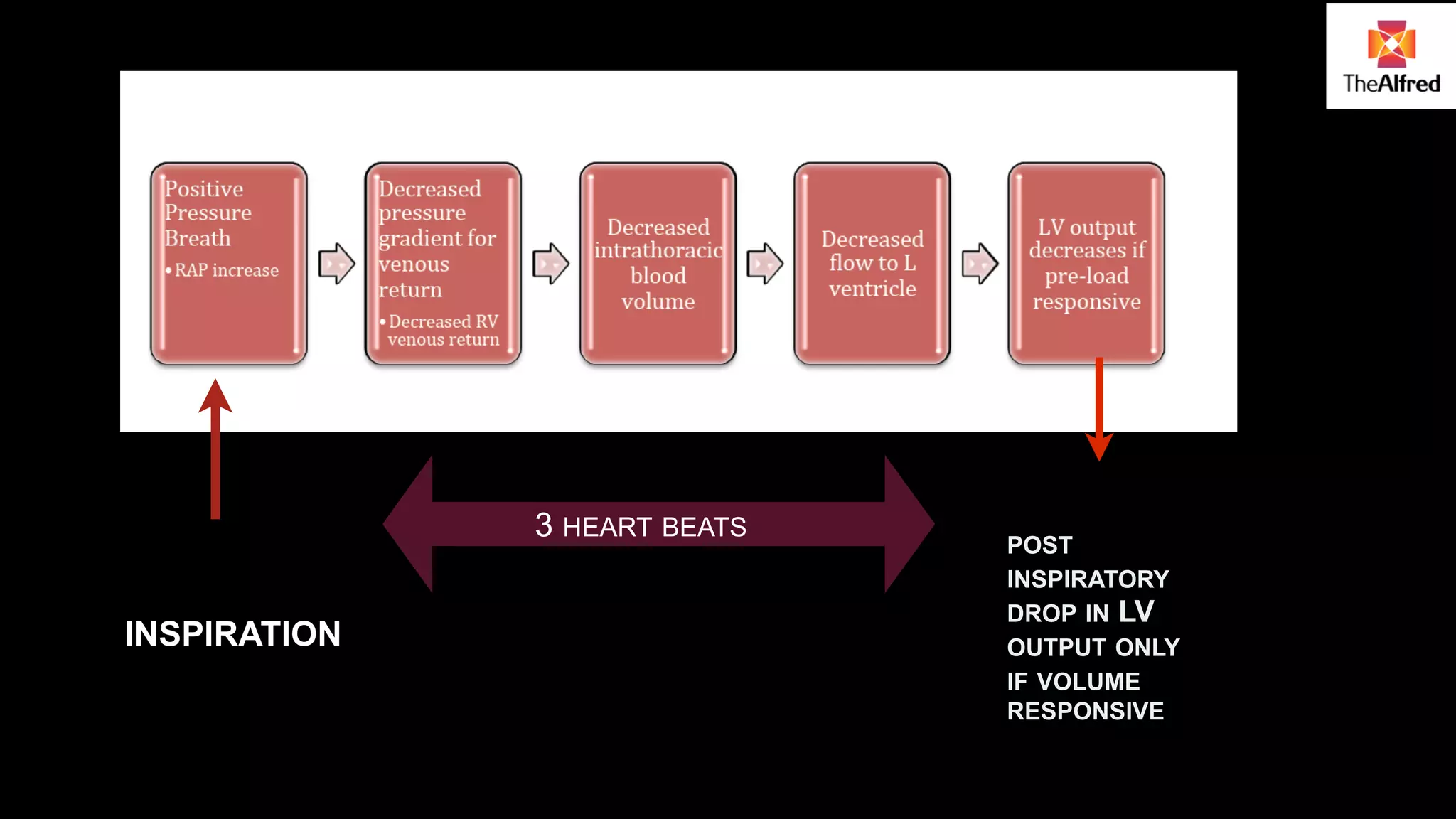
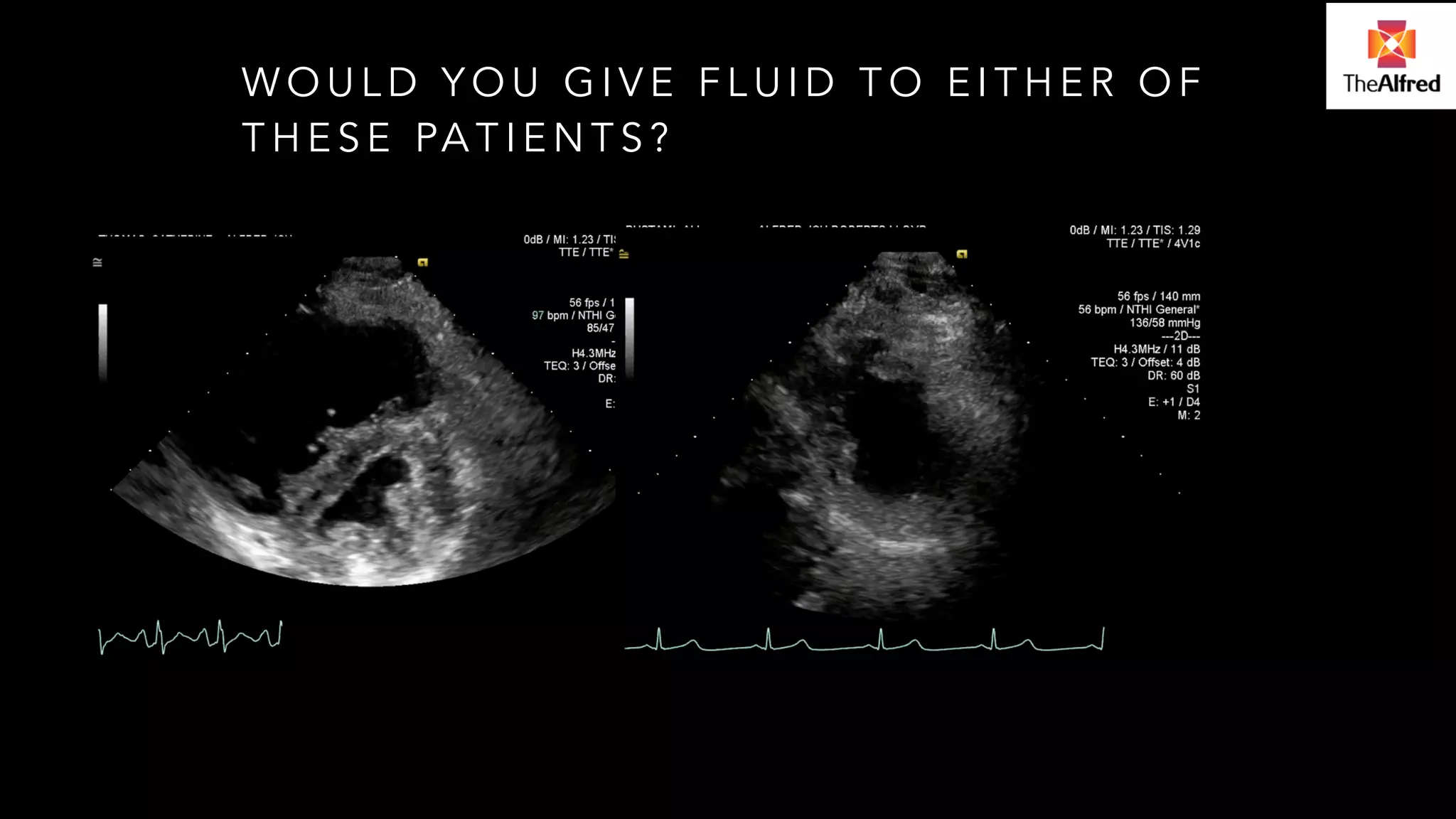
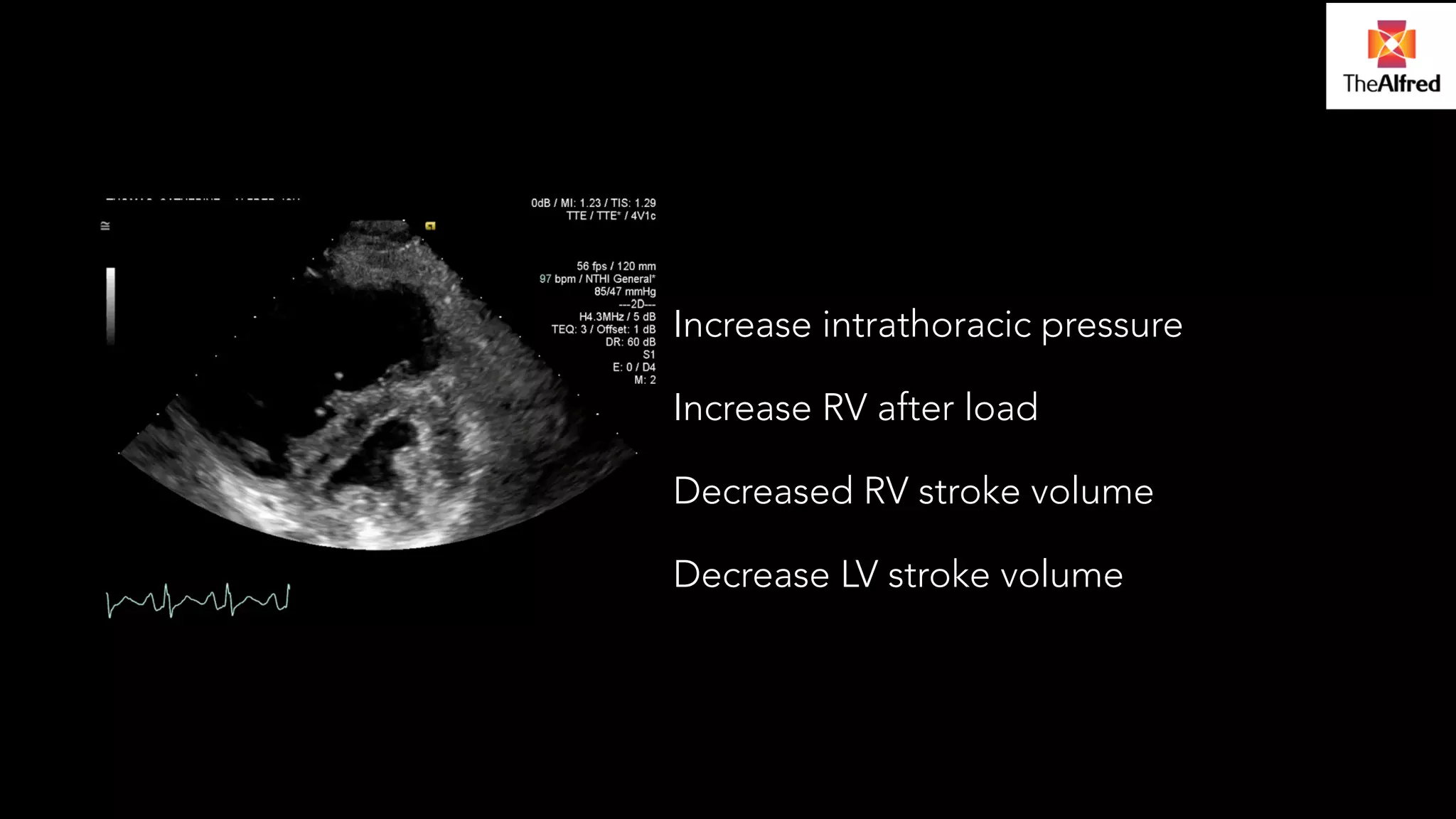
Assessment of fluid responsiveness in patients using echo to determine ventricular stroke volumes and intrathoracic pressure effects.
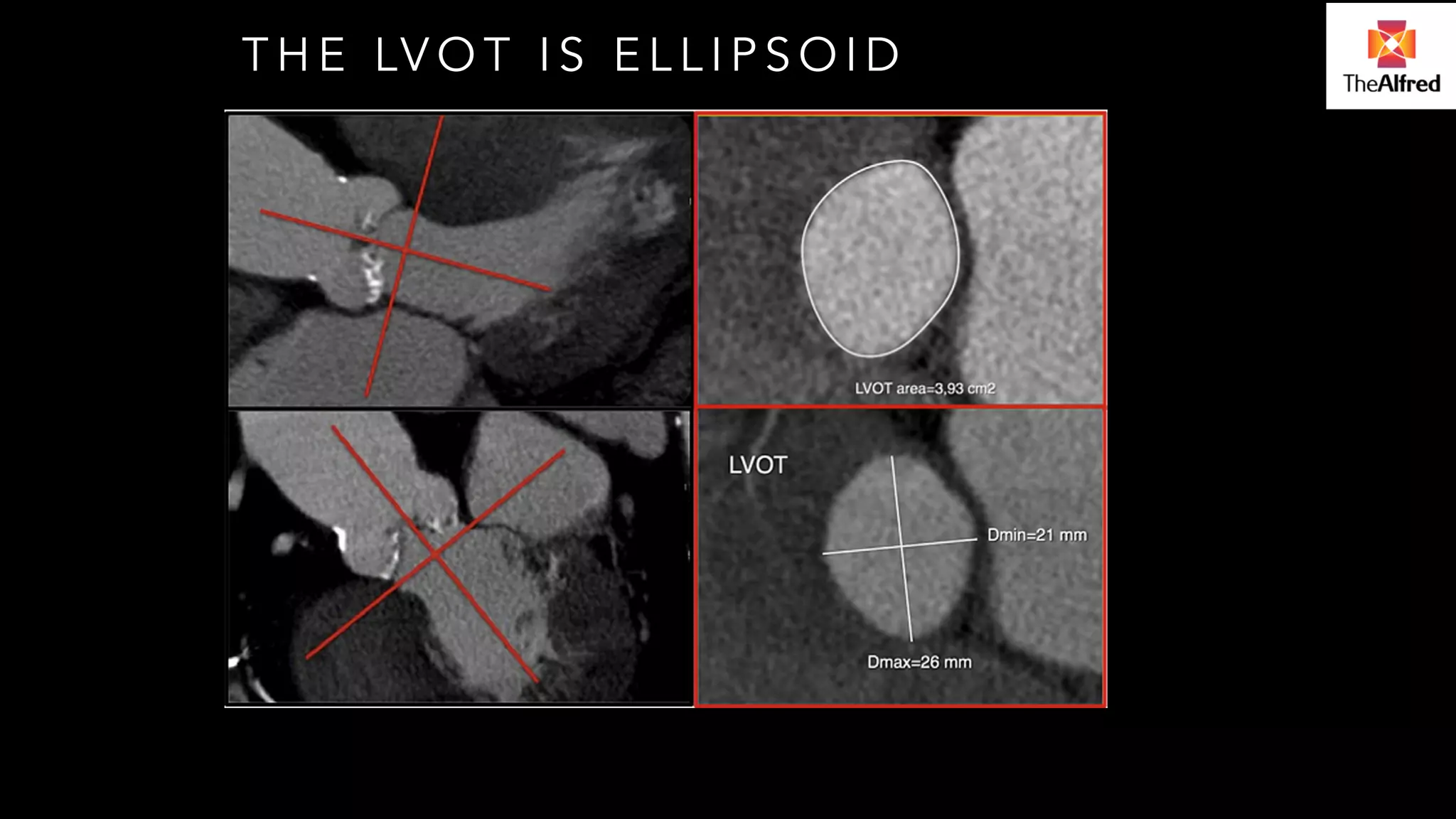
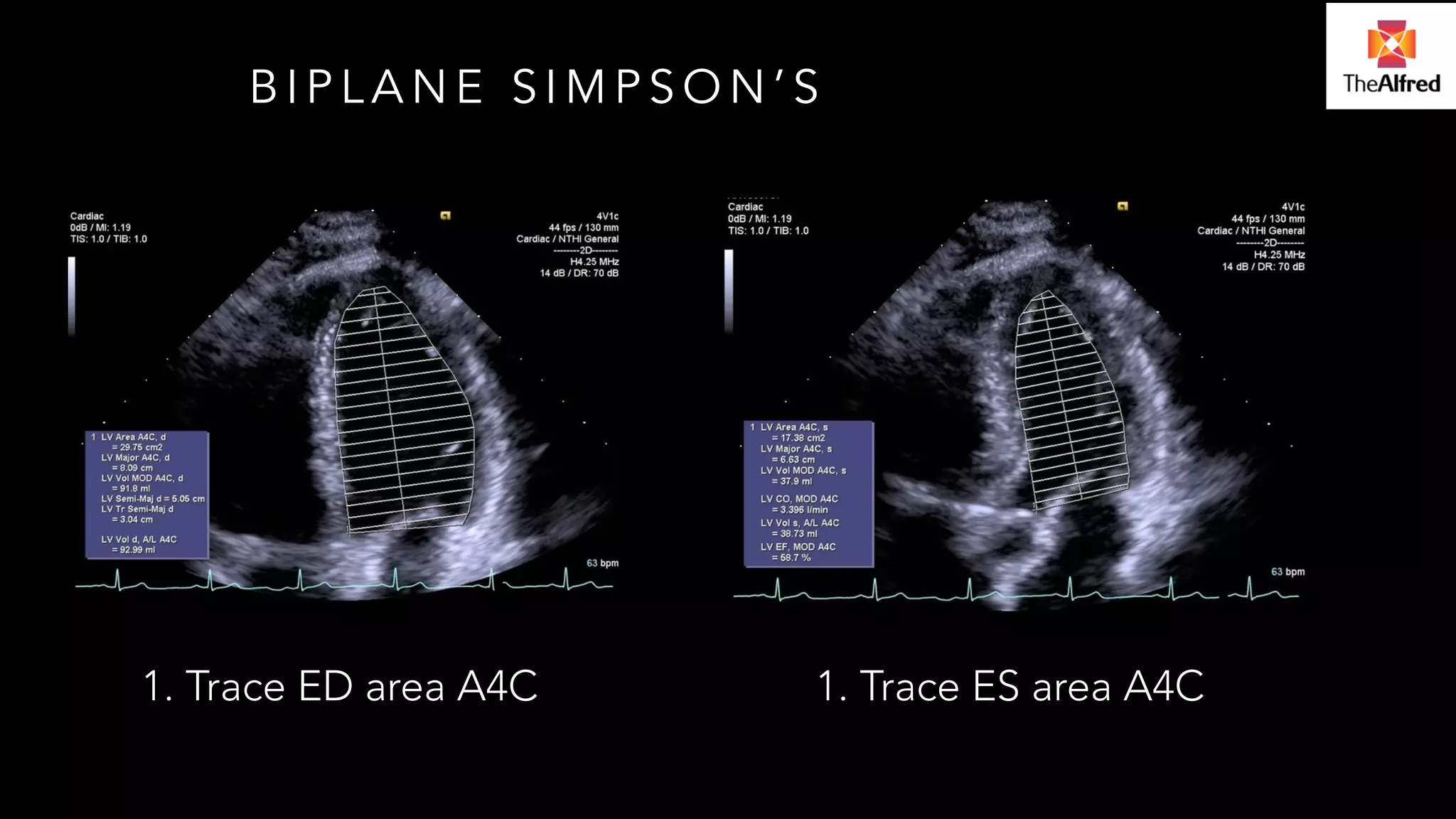
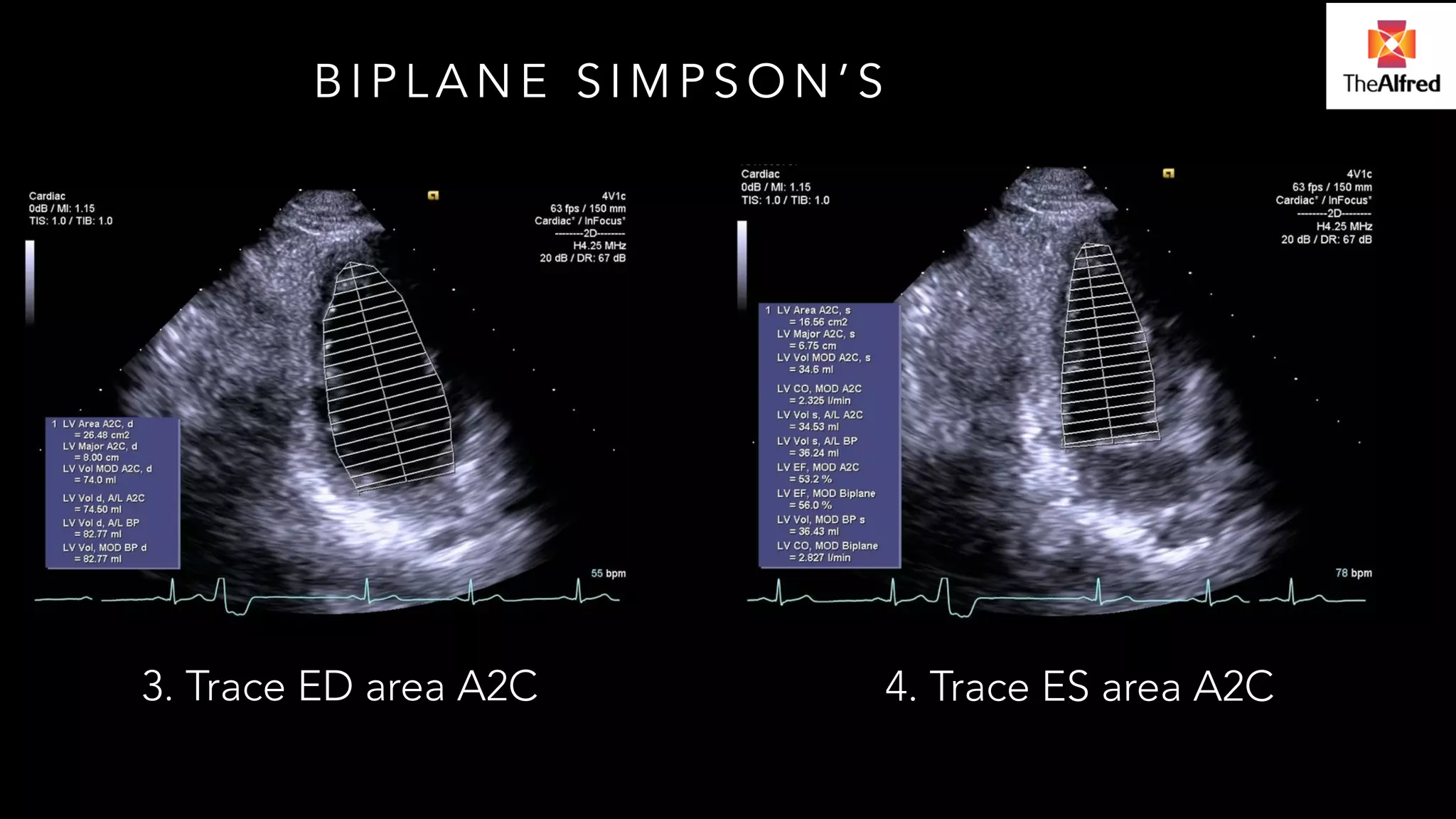
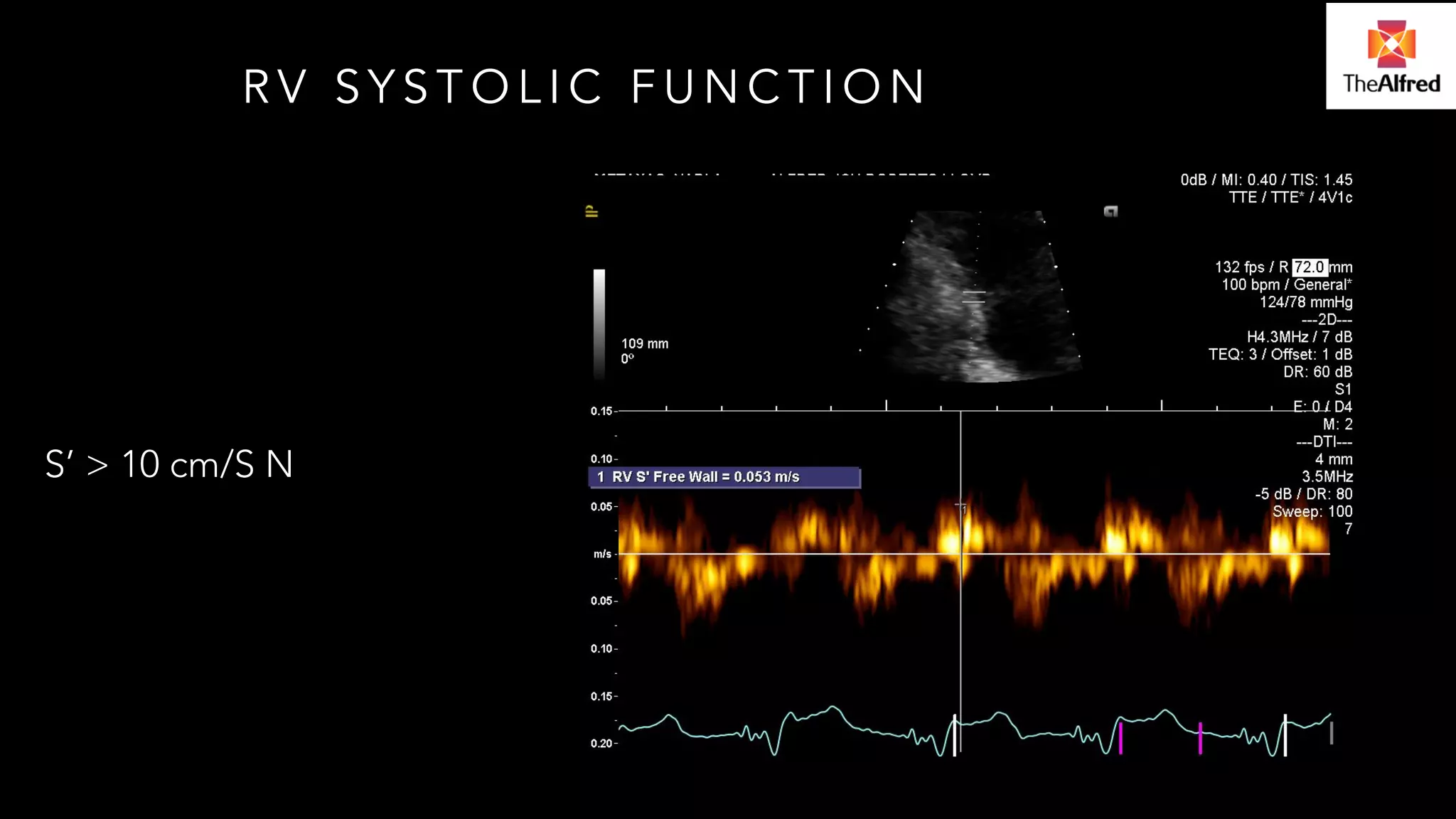
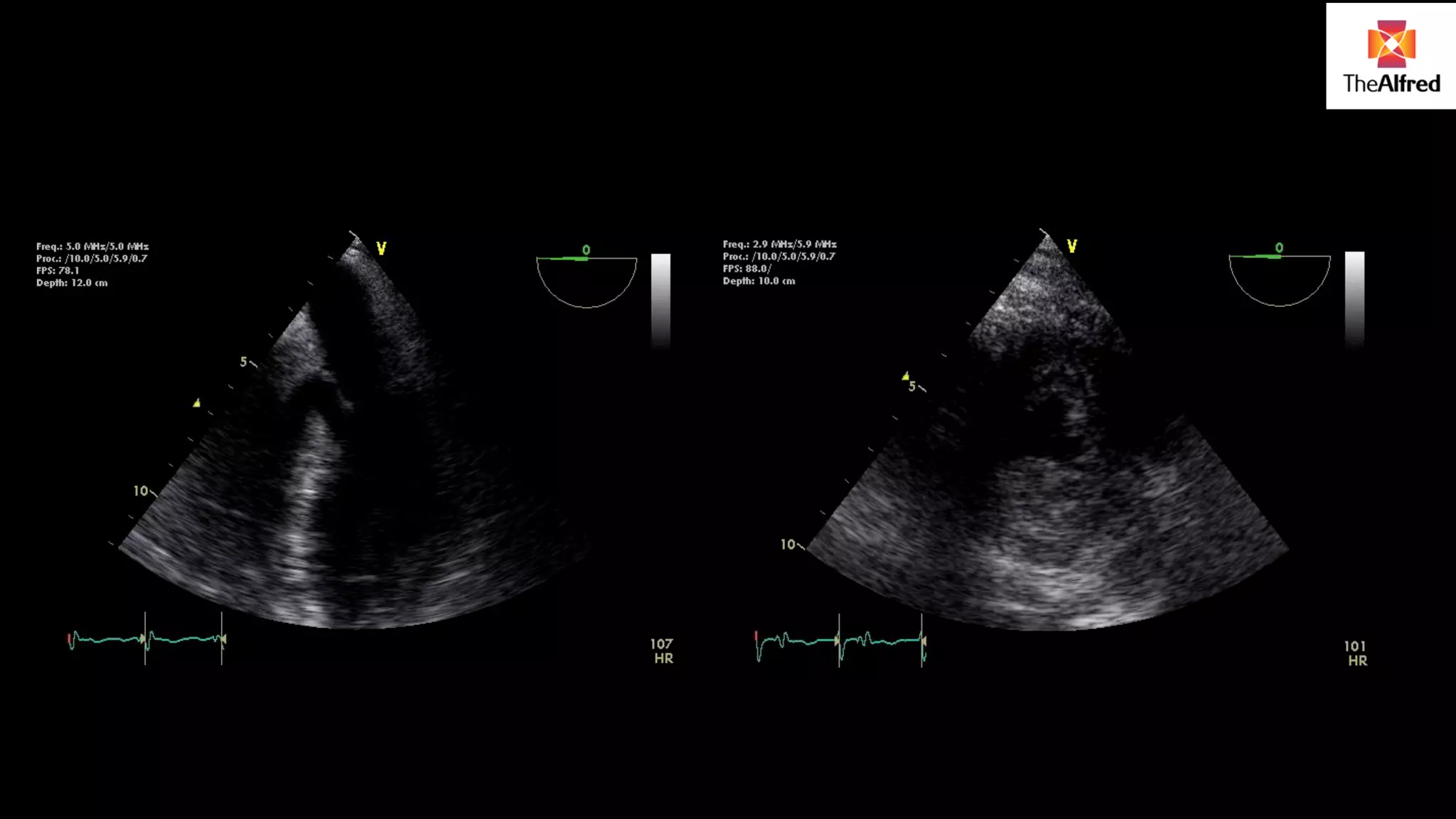
Analysis of LV function, including methods, complexities of measurements, and echocardiography as a dynamic hemodynamic tool.
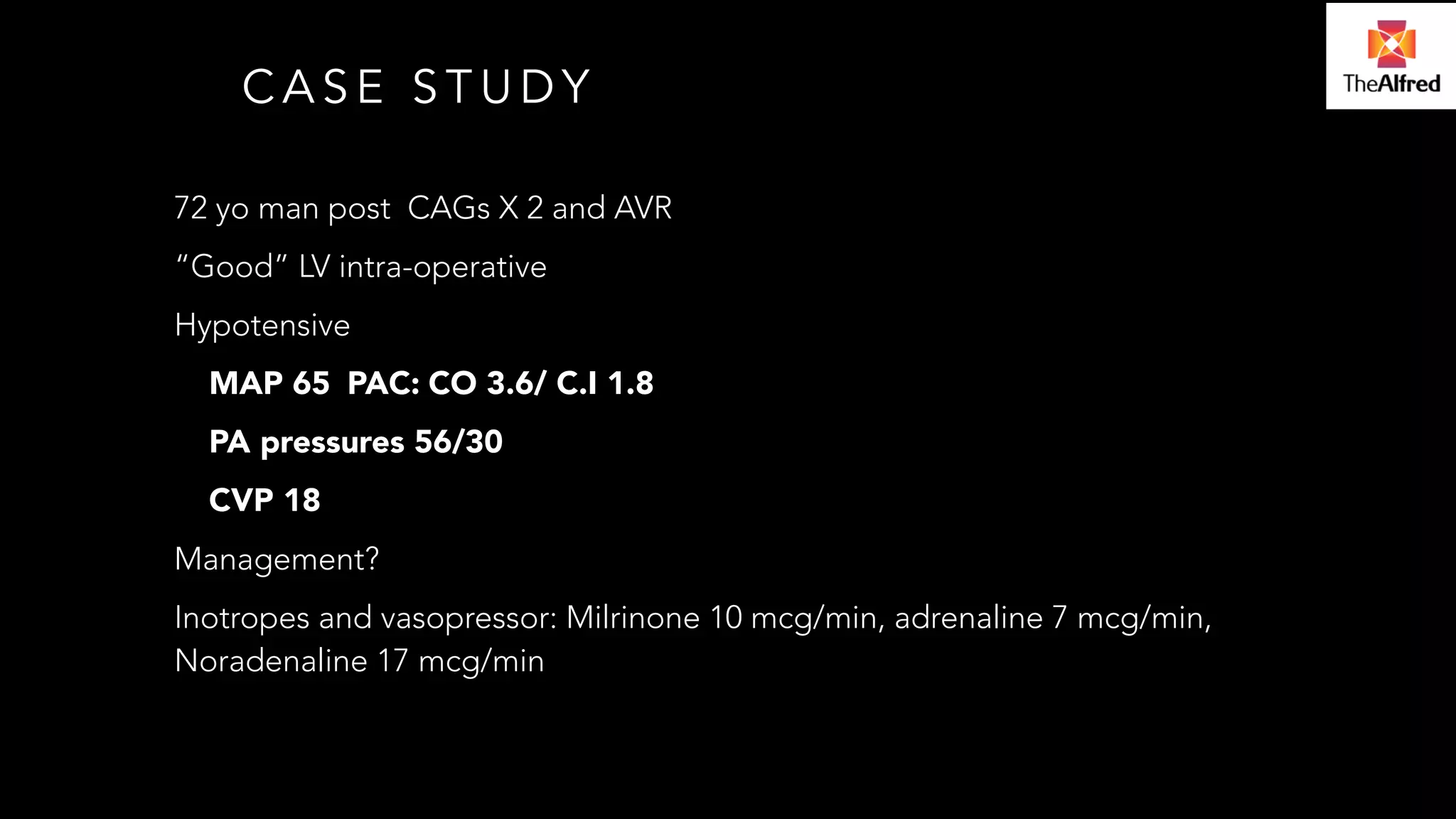
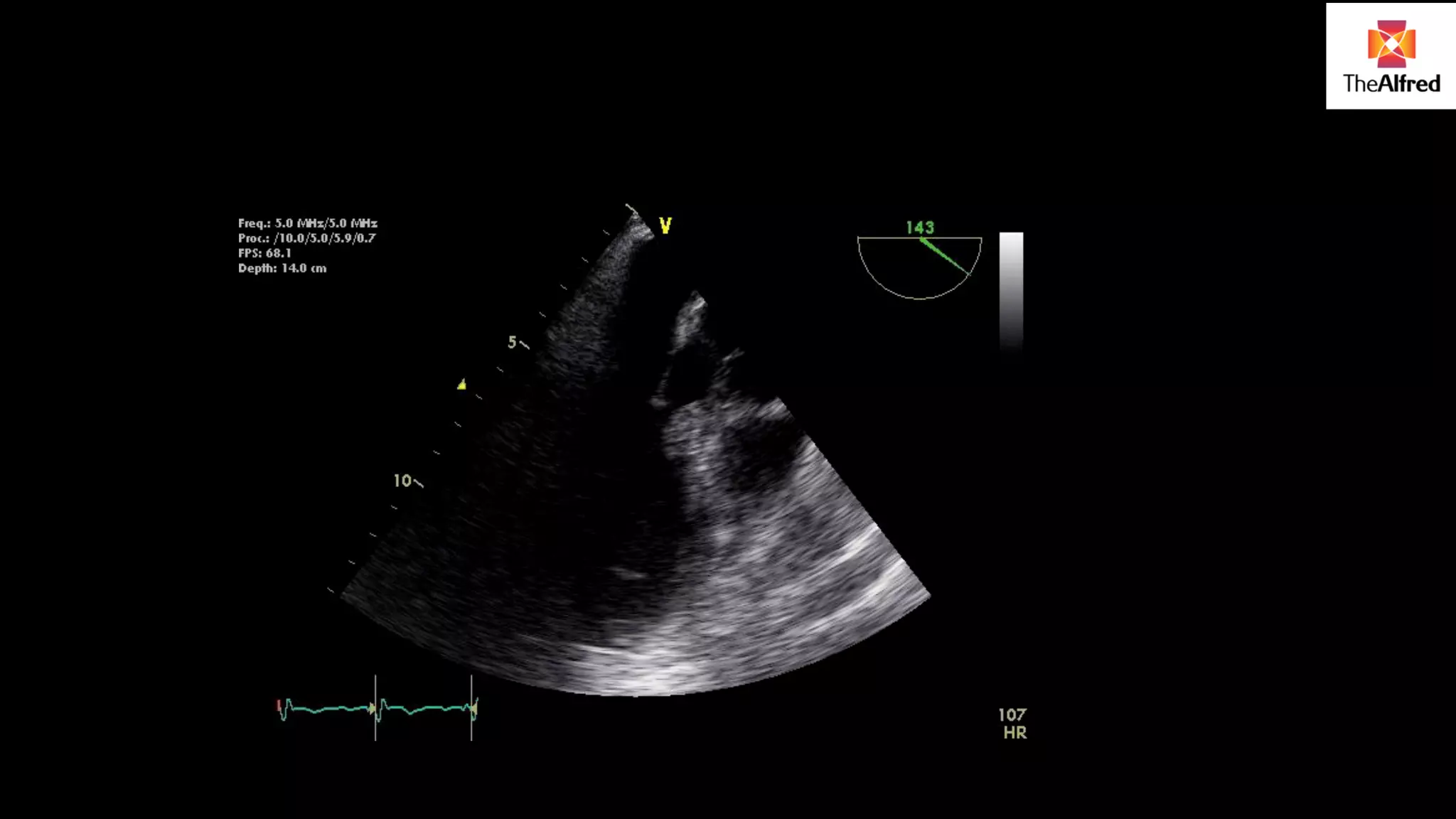
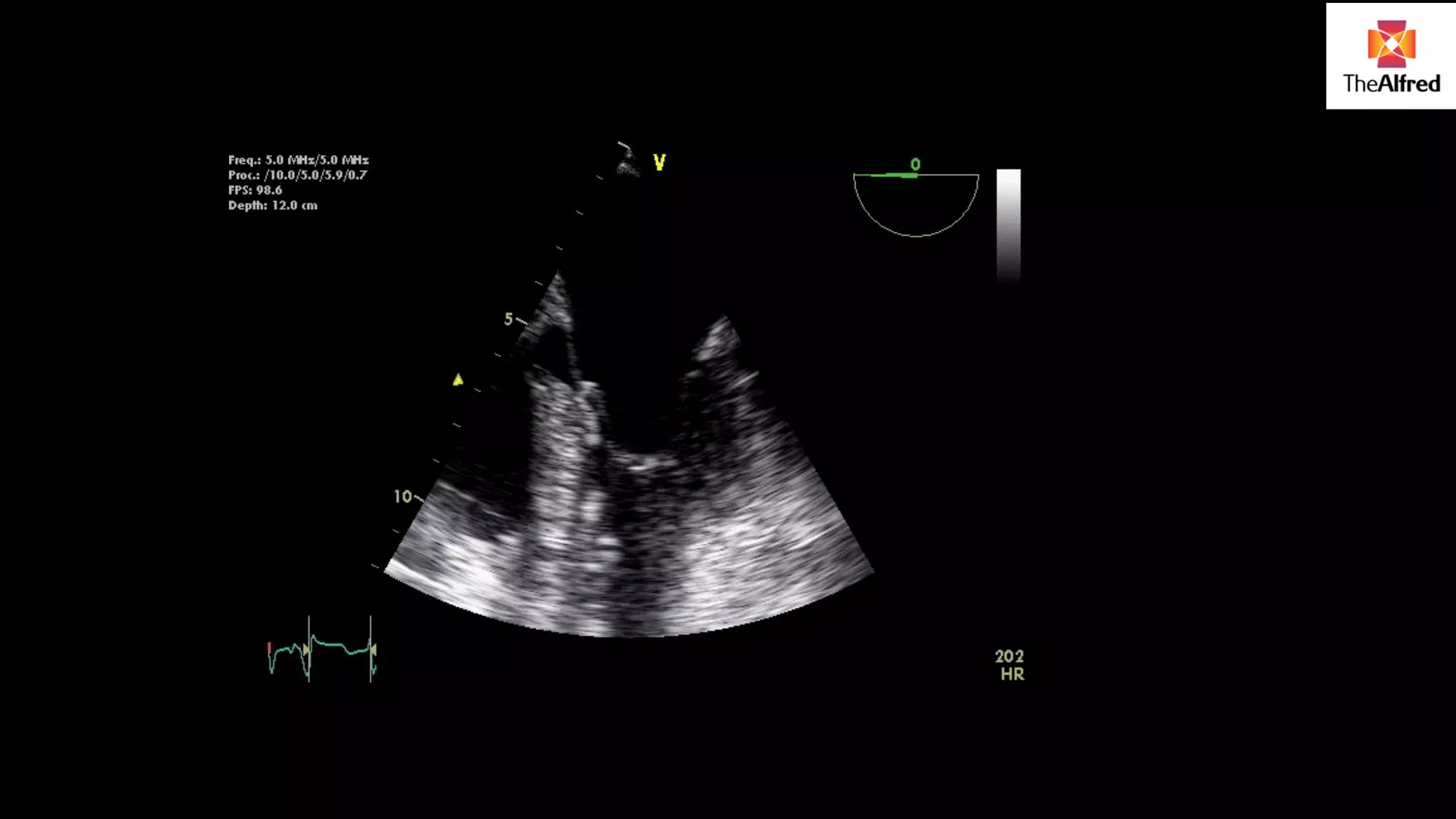
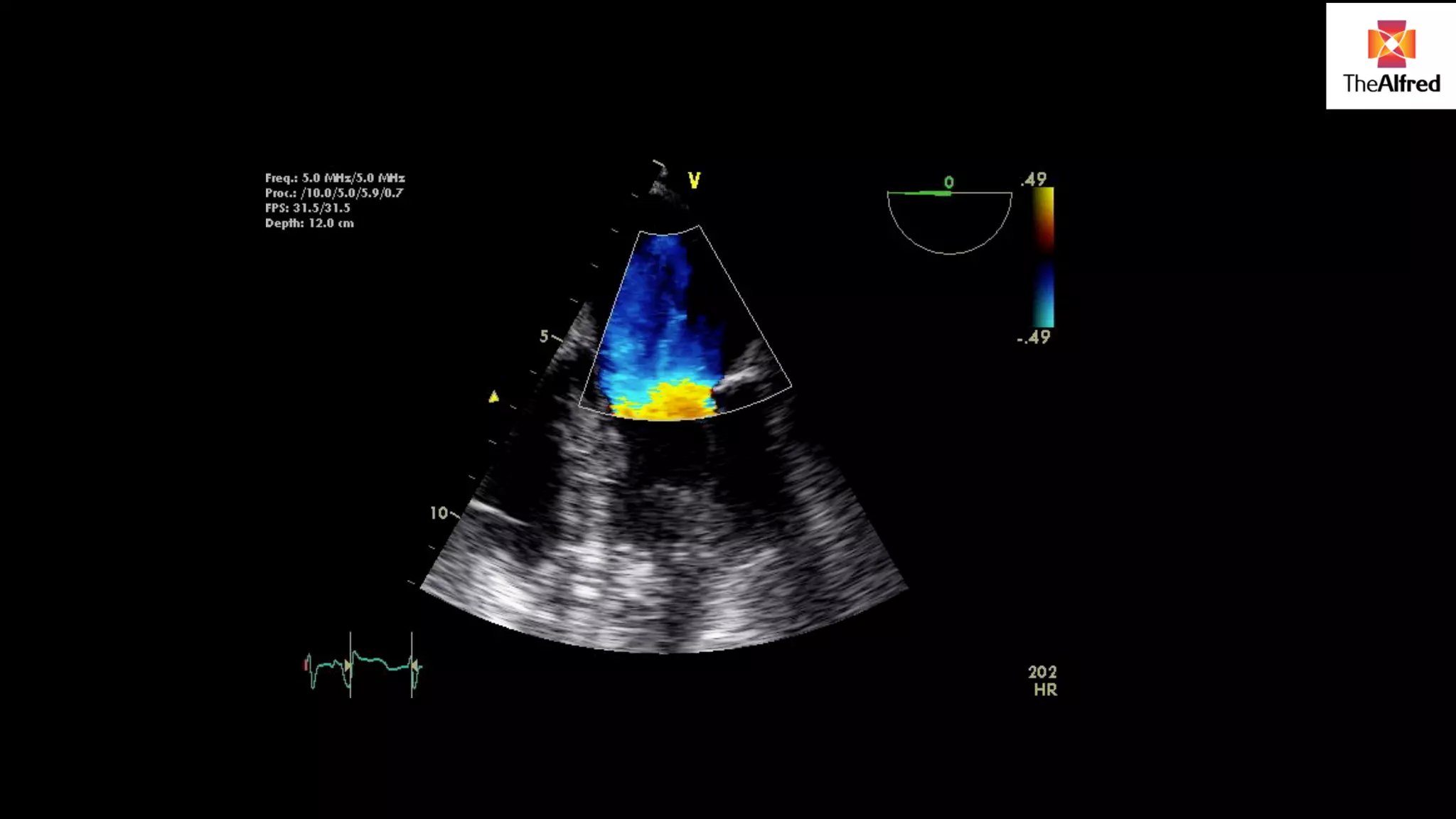
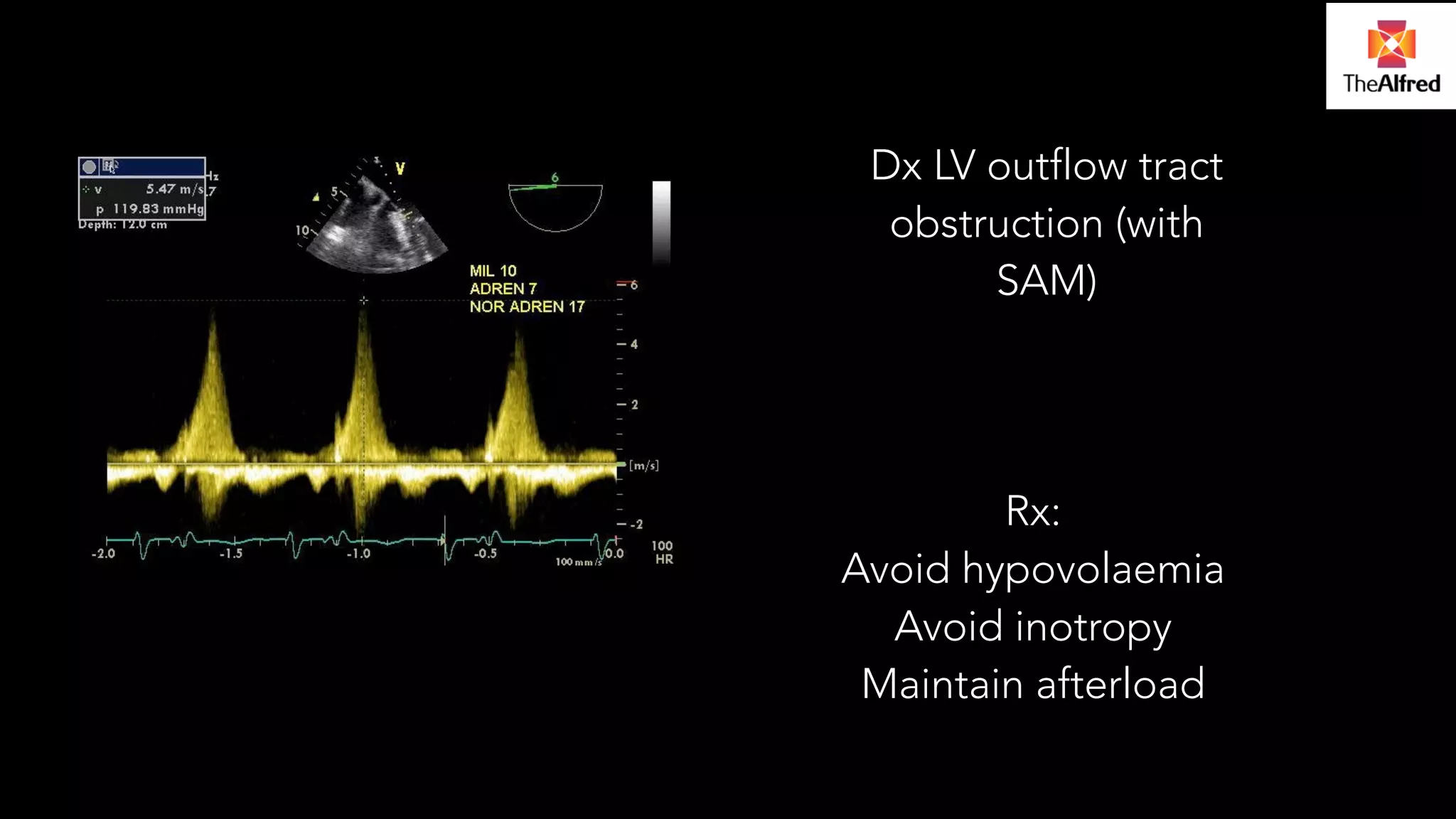
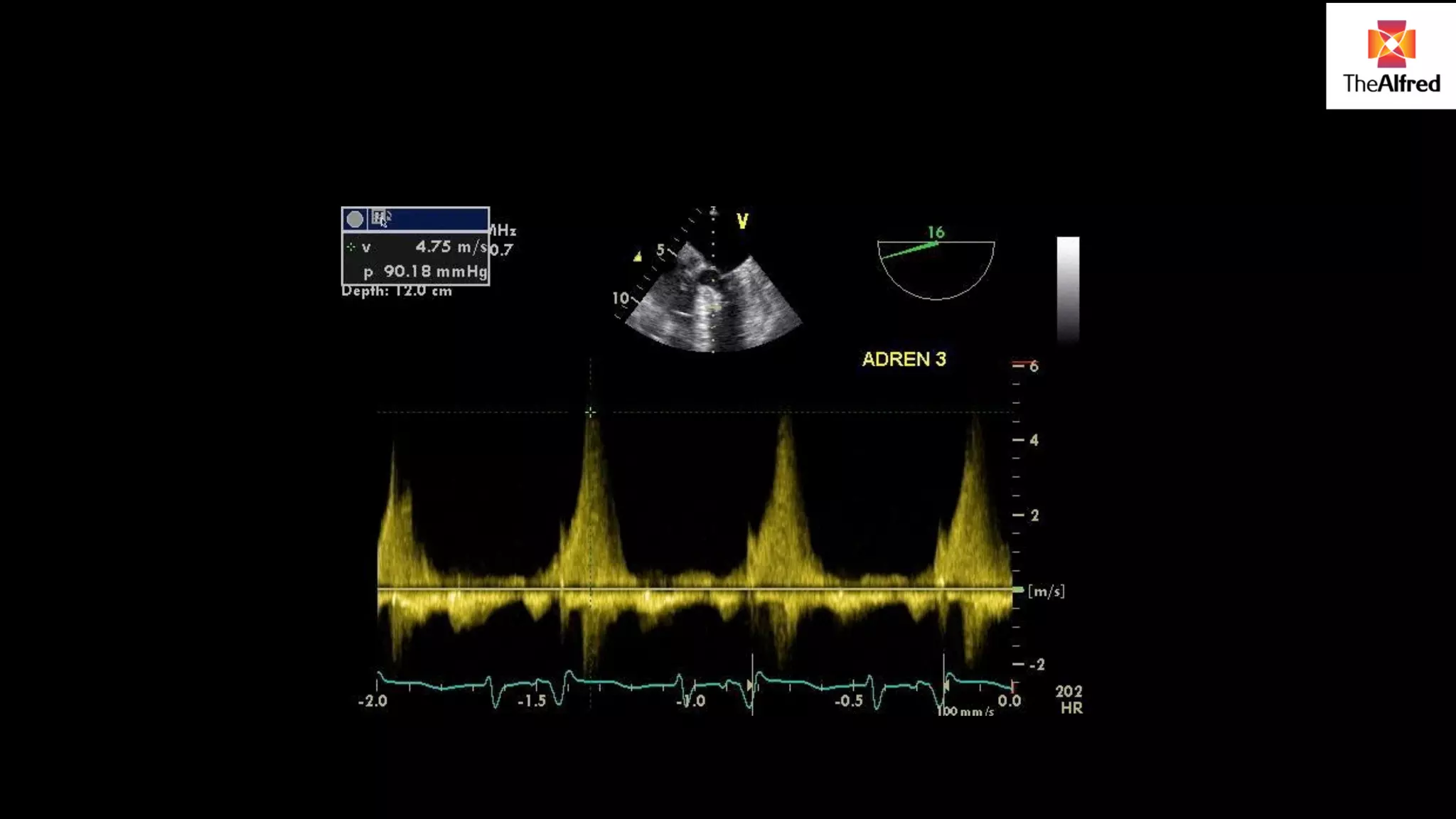
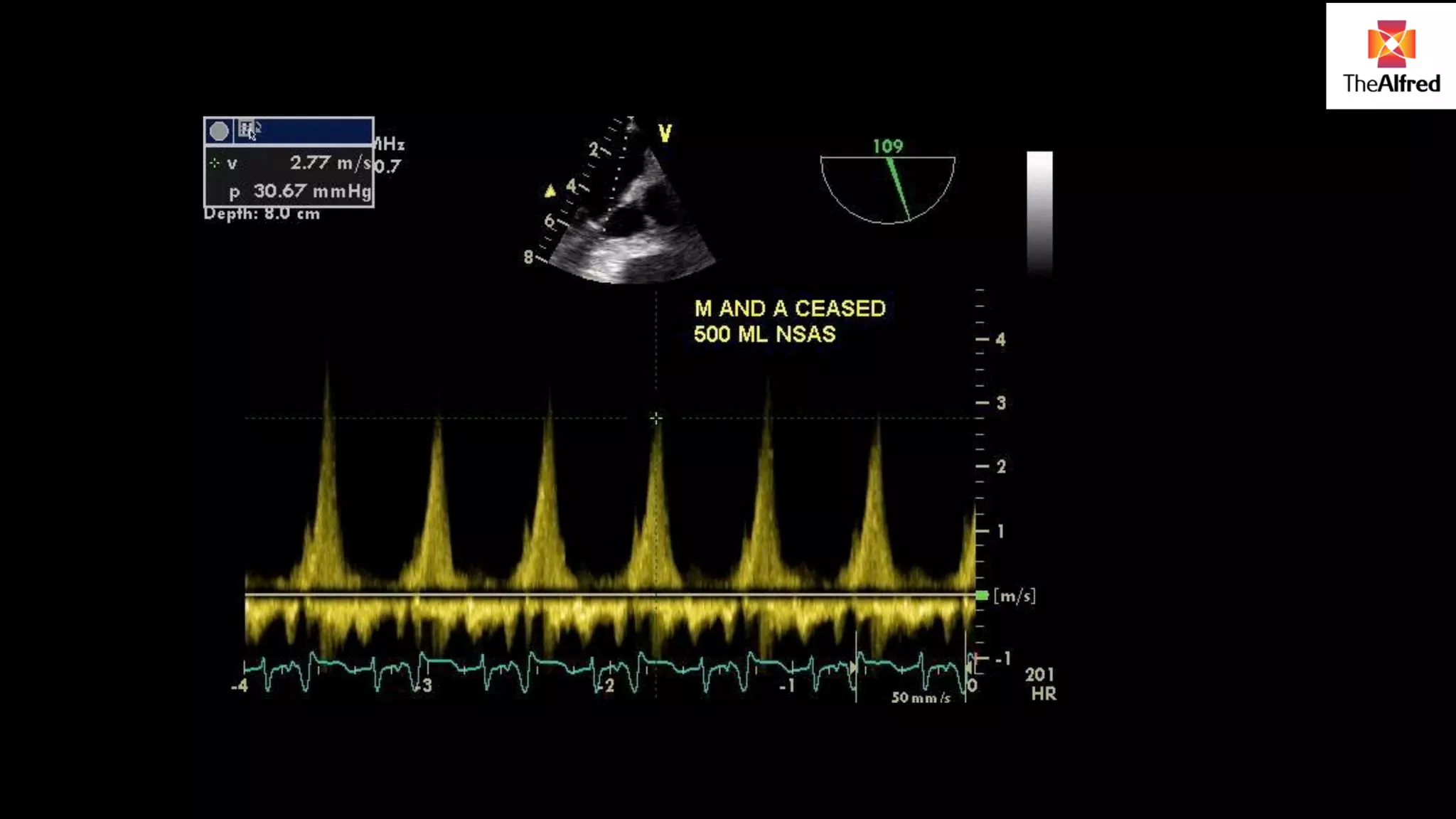
Presents a case study of a patient post-surgery, discussing differential diagnosis and the role of echo in hemodynamic management.























































































