Download as PDF, PPTX

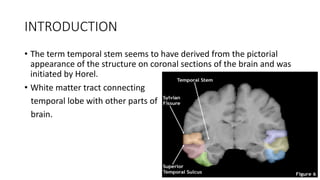









The temporal stem is a bridge of white matter in the brain connecting the temporal lobe to other regions. It contains several important tracts, including the uncinate fasciculus, inferior fronto-occipital fasciculus, and Meyer's loop. The temporal stem plays a role in functions like learning, memory, and language processing. It can also be a pathway for tumor or seizure spread. Precise knowledge of the temporal stem and its connections is important for surgical planning and understanding cognitive disorders.