Download to read offline


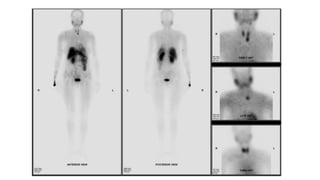

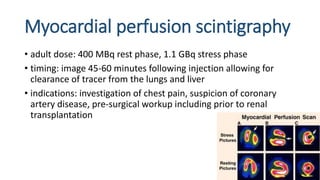

Tc-99m sestamibi is a radiopharmaceutical used for parathyroid imaging and myocardial perfusion scintigraphy, known for its uptake in metabolically active tissues. For parathyroid scans, the adult dose is 740 MBq, with imaging performed at 15 minutes and 2 hours, while myocardial perfusion scintigraphy typically uses a 400 MBq dose at rest and 1.1 GBq during stress. The technique is vital for diagnosing conditions like coronary artery disease and parathyroid adenomas, with specific imaging protocols to assess both blood flow and tissue abnormalities.