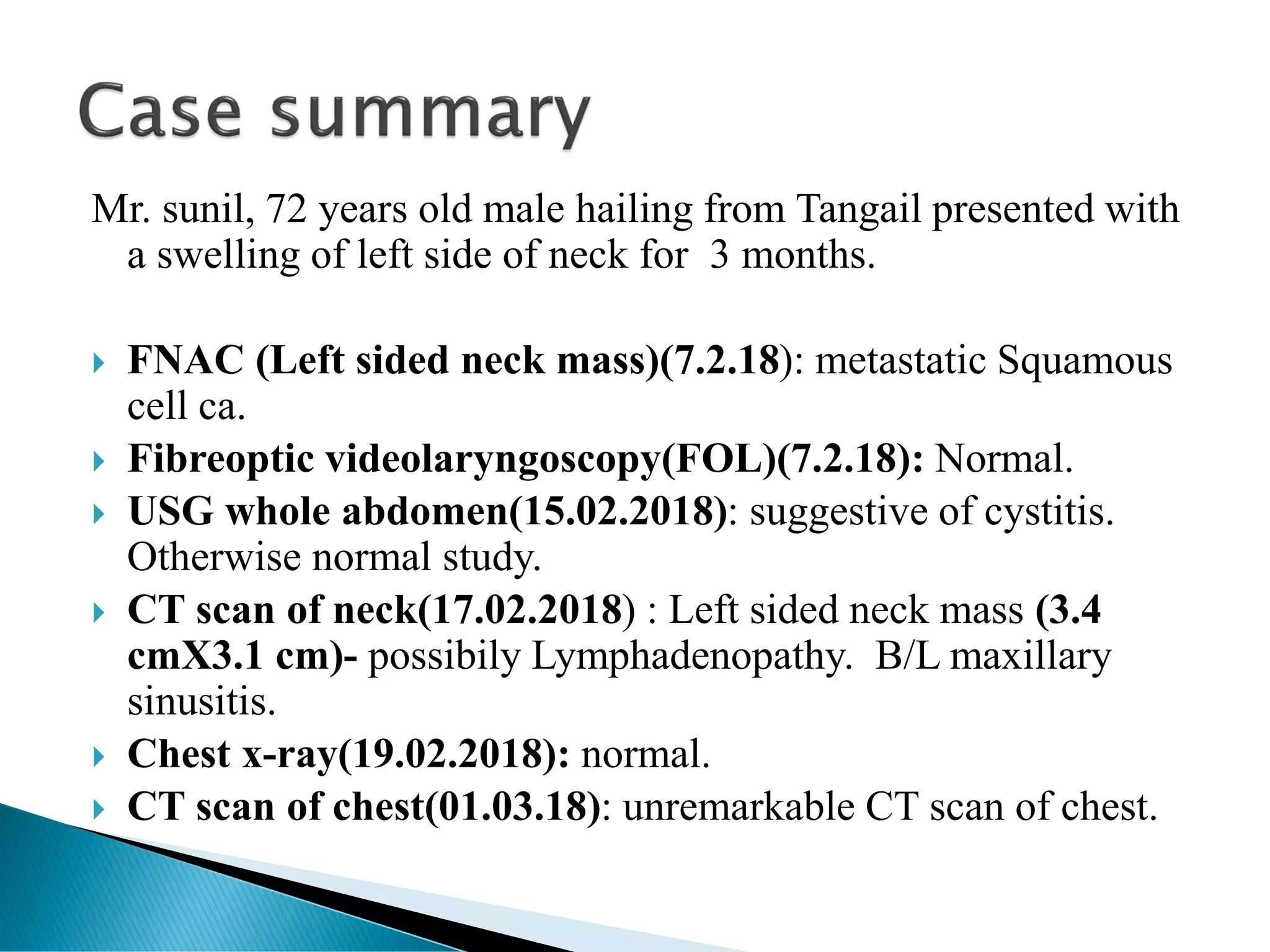
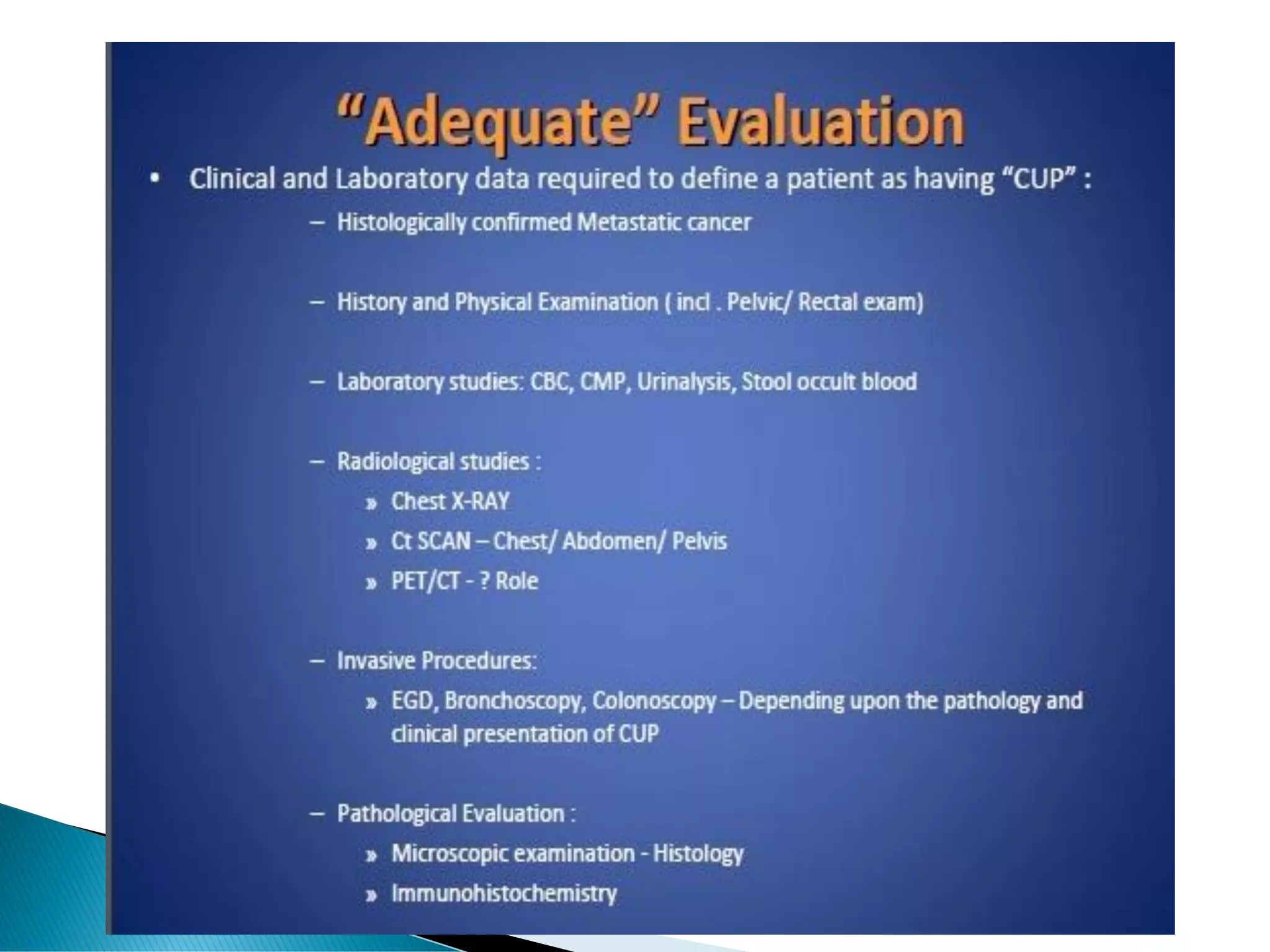
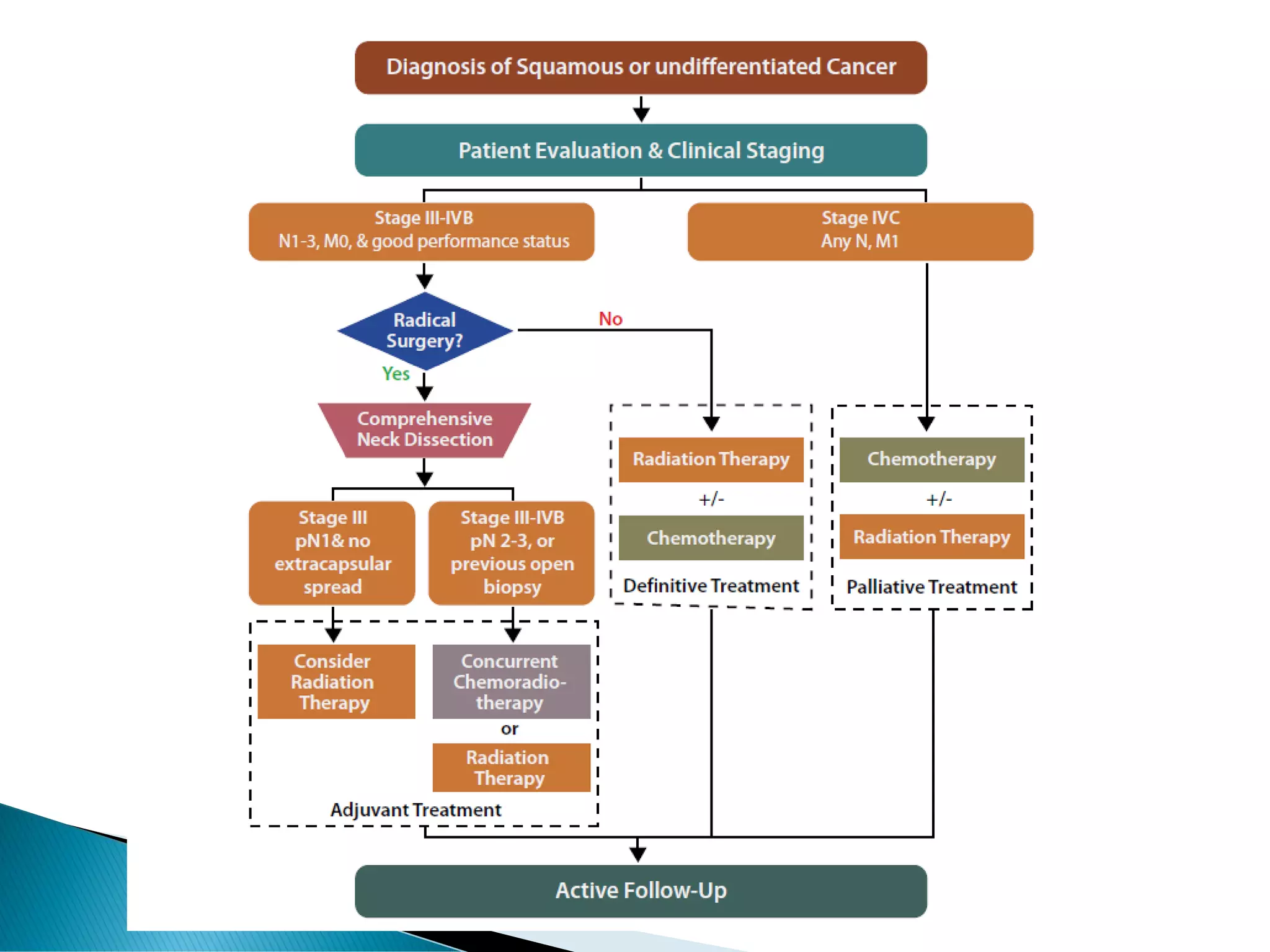
Mr. Sunil, a 72-year-old male, presented with a 3-month history of a left neck swelling. Further examinations revealed metastatic squamous cell carcinoma in the left neck lymph nodes. He was diagnosed with carcinoma of unknown primary (CUP) and underwent radical neck dissection, followed by chemotherapy and radiotherapy. CUP describes metastatic cancers where the primary site cannot be identified despite various examinations and evaluations. Treatment options for CUP include surgery, radiation therapy, chemotherapy, or concurrent chemoradiation depending on the lymph node involvement and other factors. Prognosis depends on the stage and presence of extracapsular extension, with 5-year survival rates ranging from 30% for upper cervical nodes to 5%


















































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)


















