This document provides Kenya's integrated guidelines for tuberculosis, leprosy and lung disease from 2021. It covers approaches to active case finding for tuberculosis, diagnosis and treatment of drug susceptible and drug resistant tuberculosis in adults and children. It also includes guidance on management of latent tuberculosis, tuberculosis infection control, chronic lung diseases including asthma and COPD, as well as leprosy diagnosis and treatment. The guidelines are intended to provide a comprehensive resource for healthcare workers on integrated patient-centered care for tuberculosis, leprosy and lung health in Kenya.











































































































![Integrated Guideline for Tuberculosis,
Leprosy and Lung Disease | 2021
97
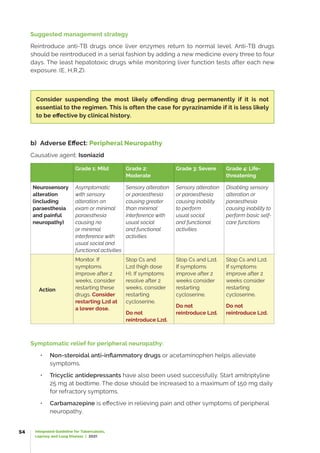
The TB-exposed neonate is highly vulnerable and may rapidly progress to symptomatic
and severeTB disease. Symptoms and clinicalsigns ofneonatalTB are usuallynonspecific
and examples are shown in the table below:
Table 4.21: Signs and Symptoms of Neonatal TB
Symptoms Clinical signs
Lethargy Respiratory distress
Fever Non-resolving ‘pneumonia’ or respiratory infection
Poor feeding Hepatosplenomegaly
Low birth weight Lymphadenopathy
Poor weight gain Abdominal distension
Clinical picture of ‘neonatal sepsis’
The diagnosis of TB should be included in the differential diagnosis of a child with
neonatal sepsis, poor response to antimicrobial therapy, congenital infections, and
atypical pneumonia. The most important clue to the diagnosis of neonatal TB is a
maternal history of TB or any contact with a person with a chronic cough.
Clinical evaluation of the infant in the setting of suspected congenital TB should include
TST and interferon-gamma release assay (IGRA), HIV testing, chest radiograph, lumbar
puncture, cultures (blood and respiratory specimens), and evaluation of the placenta
with histologic examination (including acid-fast bacilli [AFB] staining culture). The TST in
newborns is usually negative, but an IGRA test may be positive in some cases.
4.8.2 Management of the Asymptomatic Neonate Exposed to
Maternal TB
If a neonate is born to a mother with TB or is exposed to a close contact with TB, TB
Preventive Therapy (TPT) should be given for 6 months once TB disease has been ruled
out. BCG can be given 2 weeks after completion of TPT. It is not necessary to separate
the neonate from the mother. However, the mother should be educated on infection
prevention control measures.
Breastfeeding is not contraindicated for a child whose mother has TB
Neonates born to mothers with MDR-TB or XDR-TB should however be referred for TB
screening and management. TPT should not be given. Infection control measures such
as the mother wearing a mask are required to reduce the likelihood of mother to child
transmission of DR TB.](https://image.slidesharecdn.com/tbguidelines-2021-final-230131152514-1054a7a0/85/TB-Guidelines-2021-Final-pdf-113-320.jpg)







































































































































![Integrated Guideline for Tuberculosis,
Leprosy and Lung Disease | 2021
234
Appropriate Disinfectants: Phenolic agents (5% phenolin water or a phenolic disinfectant
product diluted as per label) are excellent disinfectants for cleaning up sputum spills
and for decontaminating equipment and single use items prior to disposal. Fresh
household bleach (5% sodium hypochlorite) diluted 1:10 with water can also be used as
a general disinfectant. Bleach solution works well for cleaning up blood spills; however,
it is somewhat less effective than phenolic agents against TB. It is important that bleach
dilutions be made fresh since it loses potency with time. 70% alcohol is a good agent for
cleaning bench tops.
Safe disposal of infectious waste
After smears have been processed, place all infected materials including closed sputum
containers in a biohazard bag (polyethylene, if available). Discard applicator sticks
used for smearing immediately after use. Since all sputum specimens are considered
potentially infectious, treat all materials in the procedure as contaminated.
Discard specimens by one of the following methods:
•● Incineration
•● Burying
•● Autoclaving
To protect the surrounding population, the laboratory must dispose of waste safely.
Incineration is usually the most practical way for safe destruction of laboratory waste.
If incineration cannot be arranged, discard the waste in a deep pit of at least 1.5-meter
depth. If an autoclave is available, place infected materials inside and follow procedures
for safe and adequate sterilization.
Ventilated Cabinets
Ventilated Cabinets include Laboratory Fume Hoods and Biological Safety Cabinets.
The details of these devices follow.
1. Laboratory Fume Hoods
The least expensive ventilated cabinet for laboratories is the Laboratory Fume Hood.
This type of environmental control is designed for the purpose of worker protection (no
protection of the environment or the product [specimen/ culture]). These devices, like
Biological Safety Cabinets, are designed to minimize worker exposures by controlling
emissions of airborne contaminants (including aerosols) through the following:
• The full or partial enclosure of a potential contaminant source
• The use of airflow velocities to capture and remove airborne contaminants near
their point of generation.
• The use of air pressure relationships that define the direction of airflow into the
cabinet](https://image.slidesharecdn.com/tbguidelines-2021-final-230131152514-1054a7a0/85/TB-Guidelines-2021-Final-pdf-250-320.jpg)























































![Integrated Guideline for Tuberculosis,
Leprosy and Lung Disease | 2021
290
• Give short course oral prednisone 40mg daily for 7 days if patient has severe
COPD
• High dose (800pg) inhaled corticosteroids are effective in patients with severe
COPD with more than 2 infective exacerbations per year
• Give influenza vaccine yearly and pneumococcal vaccine 5 yearly
• Identify and manage complications. Treat fluid retention with a low dose diuretic.
• Encourage patient to exercise daily e.g. walking, gardening, household chores,
using stairs instead of lifts etc.
• Review patients every 3-6 months if stable.
13.3 Post-Tuberculosis Lung Disease (PTLD)
The World Health Organization (WHO) estimates that 1.7 billion people are infected
with M. tuberculosis globally and approximately 54 million people survived Tuberculosis
(TB) between 2000 and 2017 alone. Kenya for instance notified 96,478 patients with TB
in 2018 and successfully treated 84% of them. There is increasing evidence of long-
term respiratory complications following TB in a proportion of these patients affecting
their quality of life. For many persons with tuberculosis, a microbiological cure is the
beginning, not the end of their illness.
Post TB Lung Disease (PTLD) is defined as chronic respiratory abnormality with or without
symptoms attributable, at least in part, to previous pulmonary TB.
There is evidence that over 60% of patients still have symptoms after completion
of TB treatment, over 80% have radiological sequalae, over 30% have spirometric
function test abnormalities and over 40% have bronchiectasis (Meghji J, et al 2020
[https:/
/thorax.bmj.com/content/75/3/269]).
Patients with PTLD may present with persistence of symptoms or decline in lung function
despite successful completion of treatment or cure.
Patients presenting with respiratory complaints and have recently completed
TB treatment (and who may be erroneously considered as TB relapse) should
be thoroughly evaluated for post-TB lung disease and/ or other forms of lung
conditions.](https://image.slidesharecdn.com/tbguidelines-2021-final-230131152514-1054a7a0/85/TB-Guidelines-2021-Final-pdf-306-320.jpg)








![Integrated Guideline for Tuberculosis,
Leprosy and Lung Disease | 2021
299
Table 13.13: Signs and Symptoms of Aspergillosis
Type of illness Signs / symptoms Predisposing condition
Allergic reaction
(allergic
bronchopulmonary
aspergillosis)
●• Fever
●• A cough that may bring up blood
or plugs of mucus
●• Worsening asthma
Develops in asthma or cystic
fibrosis
Aspergilloma ●• Normal initially
●• A cough that often brings up
blood (haemoptysis)
●• Wheezing
●• Shortness of breath
●• Unintentional weight loss
●• Fatigue
Emphysema, tuberculosis or
advanced sarcoidosis,
Invasive aspergillosis
(Most severe form and
fatal)
Signs and symptoms depend on
which organs are affected, Generally:
• Fever and chills
• A cough that brings up blood
(haemoptysis)
• Shortness of breath
• Chest or joint pain
• Headaches or eye symptoms
• Skin lesions
In people whose immune systems
are weakened as a result of
cancer chemotherapy, bone
marrow transplantation or a
disease of the immune system to
the brain, heart, kidneys or skin
Table 13.14 Diagnosis of Aspergillosis
Diagnostic spectrum
Allergic bronchopulmonary aspergillosis
(ABPA)
Invasive aspergillosis
(Chronic necrotizing
Aspergillus pneumonia)
Aspergilloma
Laboratory testing
Major:
Blood: CBC for Eosinophilia.
-Skin test - positive result for A. fumigatus
-Marked elevation of the serum
immunoglobulin E (IgE) level to greater than
1000 IU/dL
- Aspergillus Precipitin test: positive
results for Aspergillus precipitins (primarily
immunoglobulin G [IgG], but also
immunoglobulin A [IgA] and immunoglobulin
M [IgM])
Demonstration of the
organism in sputum](https://image.slidesharecdn.com/tbguidelines-2021-final-230131152514-1054a7a0/85/TB-Guidelines-2021-Final-pdf-315-320.jpg)





















































































































































































![Kyasanur forest disease477[1]](https://cdn.slidesharecdn.com/ss_thumbnails/kyasanurforestdisease4771-200524052310-thumbnail.jpg?width=640&height=640&fit=bounds)
























































