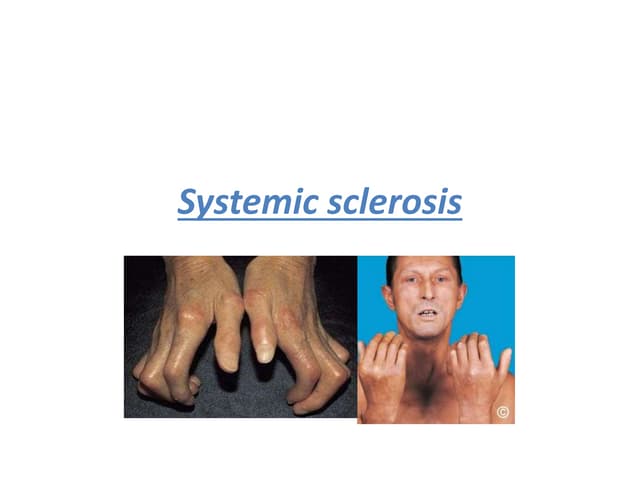
Systemic sclerosis is an autoimmune disease characterized by fibrosis of the skin, internal organs, and blood vessels. It can cause Raynaud's phenomenon, digital ischemia, thickening and tightening of the skin, and organ involvement like lung, heart, gut, and kidney disease. The cause is unknown but likely involves genetic susceptibility and environmental triggers. It results from tissue fibrosis, blood vessel damage, and autoimmune inflammation. Treatment focuses on slowing organ damage and related complications through medications, lifestyle changes, and organ-specific interventions. Prognosis depends on organ involvement, with lung fibrosis and pulmonary hypertension being leading causes of death.