Downloaded 16 times

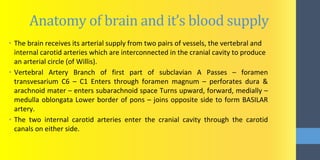
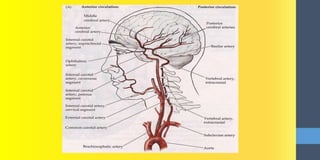
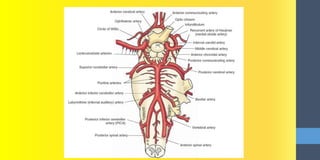
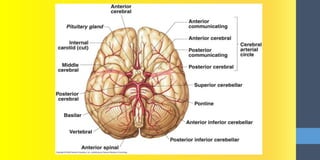
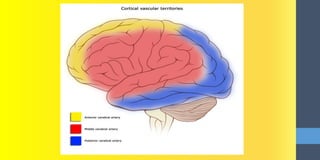
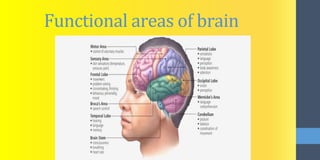
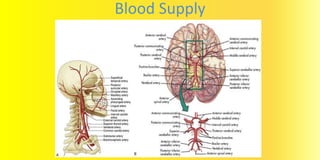
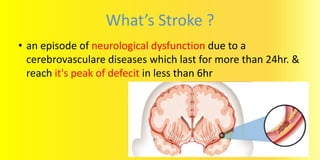


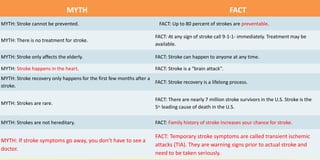


This document provides information about strokes, including: - The anatomy of the brain and its blood supply from arteries. - The definition of a stroke as a neurological dysfunction lasting over 24 hours due to cerebrovascular disease. - The types, causes, risk factors, signs and symptoms, and management of ischemic and hemorrhagic strokes. - Myths and facts about strokes, including that up to 80% are preventable but they can affect anyone at any time. It then discusses the case of a 77-year-old woman who suffered paralysis on her right side and an inability to speak after a stroke, indicating a left middle cerebral artery blockage.





![Neurocognitive Disorders [2020]](https://cdn.slidesharecdn.com/ss_thumbnails/ncd2020v2-200526001756-thumbnail.jpg?width=640&height=640&fit=bounds)





























































