Download to read offline
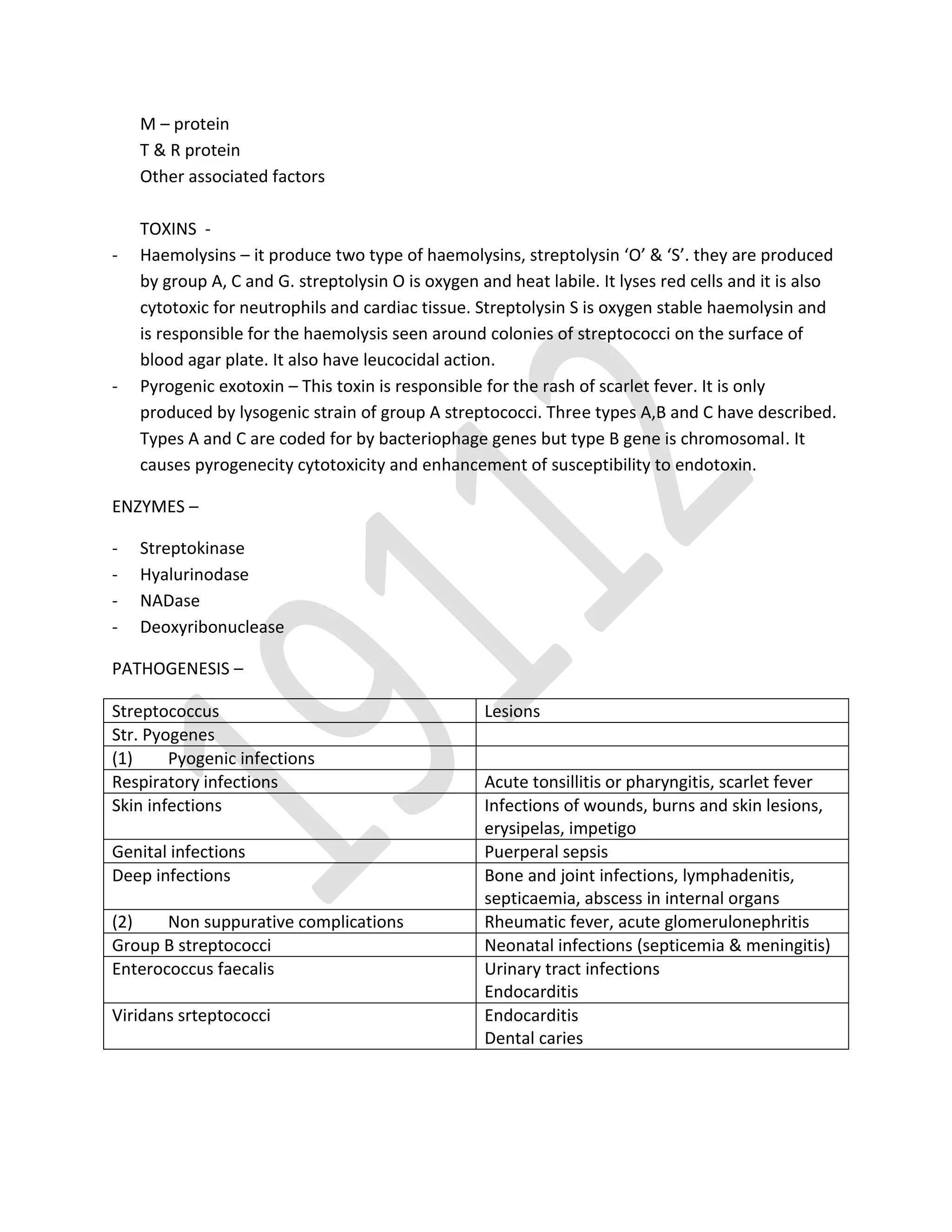


Streptococcus is a gram positive coccus that forms chains and is part of normal human flora. It is classified into alpha, beta, and gamma hemolytic streptococci based on hemolytic properties. Streptococcus pyogenes causes pyogenic infections like tonsillitis, scarlet fever, impetigo, and puerperal sepsis as well as non-suppurative complications like rheumatic fever and acute glomerulonephritis. Diagnosis involves culturing specimens on blood agar to observe characteristic colonies and conducting tests like Gram stain, biochemical reactions, and Lancefield grouping. Penicillin G is the treatment of choice for streptococcal infections.