
Download to read offline
![Results – Table 1Results – Table 1
Characteristics Cases
(N=160), [%]
Controls
(N=320), [%]
P-Value
Age 72 (66-77) 69 (62-75) <0.001
COPD 58 (36) 64 (20) <0.001
Renal failure 34 (21) 37 (12) 0.005
Angina pectoris 55 (34) 76 (24) 0.01
Myocardial infarction 84 (53) 109 (34) <0.001
Heart failure 44 (28) 35 (11) <0.001
Stroke 35 (22) 29 (9) <0.001
Type of surgery 1.0
Poldermans et al., Circulation 2003; 107: 1848-1851](https://image.slidesharecdn.com/2vpkfy8btsixnb3z6dfe-signature-185c9c8f74195a69485b096cbf5bfb73f6b3ed8b7754452e736ee4598185e9e3-poli-160919191615/85/Statins-are-associated-11-320.jpg)
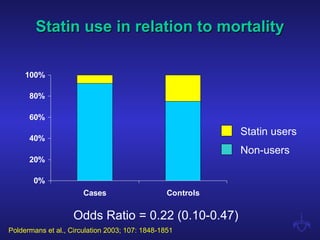
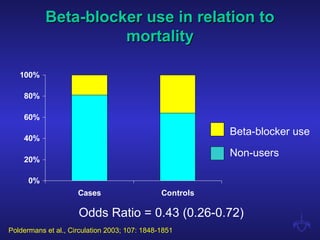
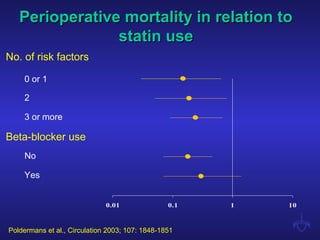
Statins are associated with a reduced incidence of perioperative mortality in patients undergoing major vascular surgery. In a retrospective case-control study of 2816 patients, statin use was associated with a 78% reduced risk of perioperative mortality. Patients taking statins had over a four-fold lower risk of death compared to non-users. The protective effect of statins was consistent regardless of cardiac risk factors or beta-blocker use.










































































































