#4 The etiology remains unclear, but assumptions such as hypertrophy of a lobe of a salivary gland, bony erosion caused by vascular compression, or an incomplete Meckel cartilage calcification during ossification, have been proposed.
#5 The SBC is also known under a myriad of synonyms:,
#6 Static bone cavity is also known as stafne cyst. However, this condition is not a cyst, but a focal cortical bone defect.
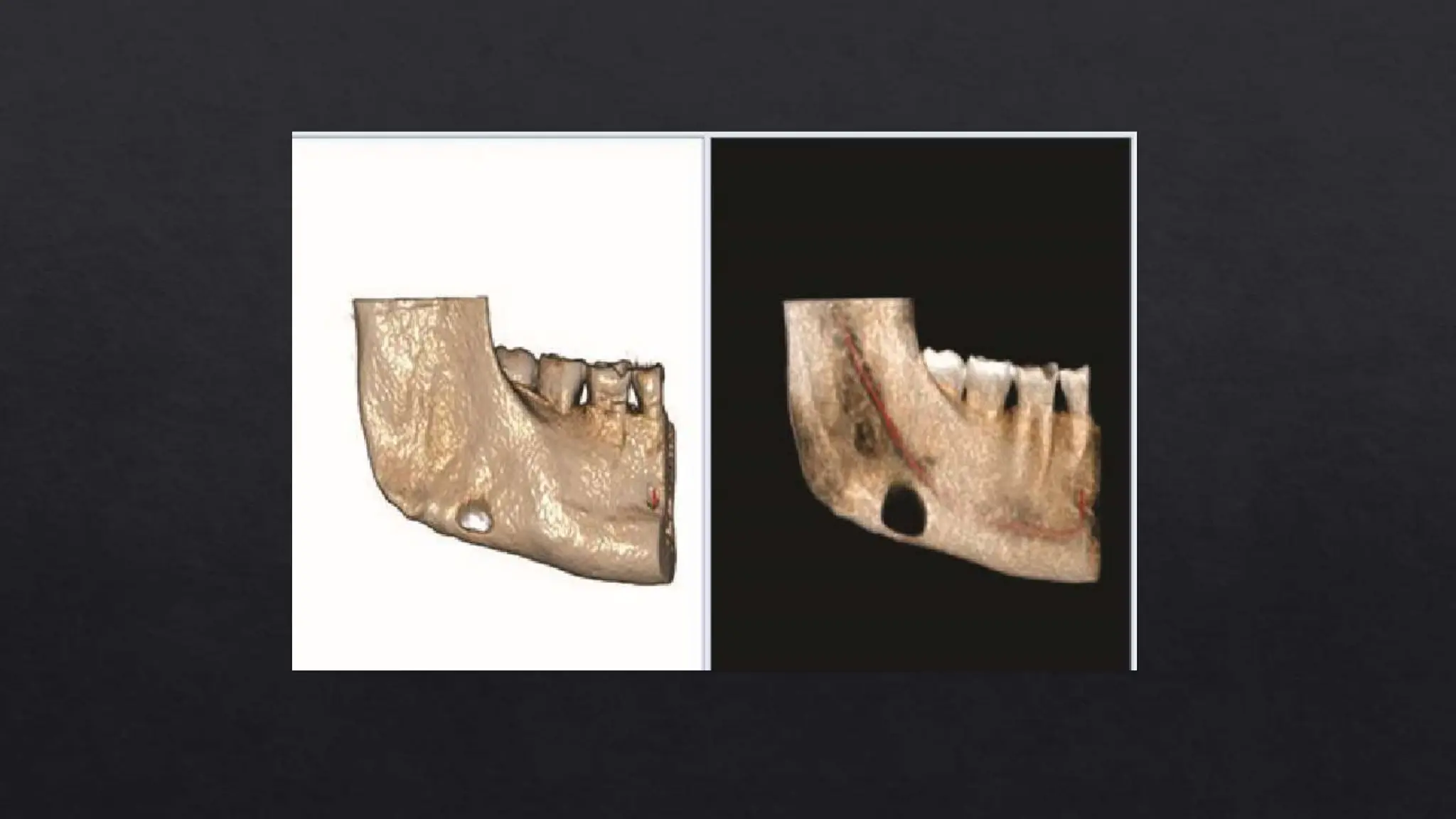
The location the lingual aspect of the angle or posterior body of the mandible, below the mandibular canal, is unique enough to make the diagnosis.
Classically it has been described that the submandibular gland tissue is seen in the defect, however often only fatty tissue is identified in the cavity.
The Stafne defect is thought to be a normal anatomical variant, as the depression is created by ectopic salivary gland tissue associated with the submandibular gland and does not represent a pathologic lesion as such.
This cavity is commonly observed on panoramic radiograph.
Indicating the invagination of cortical bone.
#8 Depression of the lingual side of mandible with unilateral radiolucent cavities located in the posterior region of the mandible, between the third molar and mandibular angle. below the inferior mandibular canal and above the mandibular base.
#11 Usually an asymptomatic lesion, it is best described as a depression of the lingual aspect of the mandibular bone. However, its radiographic features may mimic that of an intra-bony cystic or neoplastic lesion
#14 Histopathological examination is seldom necessary; however Several pathogenic theories have been suggested in relation to SBC,but the congenital malformation theory (which suggests salivary gland tissue gets entrapped within the mandible duringdevelopment) is the most universallyaccepted.
Lesions as a result of congenital malformation are typically associated with a thin but intact lingual cortex, but this is not consistent with our case.
Another theory is that of adjacent structures, such as the submandibular gland compressingthe lingual aspect of the mandible or local lymphatic infiltration, which may be the causative factor.
#15 In hematoxylin-eosin staining, the mass was consisted of pure serous glandular tissue in 100× magnification (A). Acinar cells contained zymogen granules and ductal system as intact in 200× magnification (B).
#16 Biopsied cavity contents are composed of mixed seromucinous salivary gland tissue with lymphocytic infiltration.
#17 Generally, the management of SBC should be of a conservative approach with radiographic follow‑up, and no treatment is necessary. However, surgical exploration and biopsy may be reserved for those cases simulating any other benign or malignant lesions with uncertainty in diagnoses.