Surgical Treatment ofPeptic Ulcer Disease
• The indications for surgery in PUD are (in order of decreasing
frequency) perforation, obstruction, bleeding, and intractability or
nonhealing.
• Gastric cancer must always be considered in patients with gastric
ulcer or gastric outlet obstruction.
• Today, most patients undergoing emergent operation have simple
patch of a perforated ulcer or oversewing of a bleeding ulcer.
• Traditionally, the vast majority of peptic ulcers were treated by a
variant of one of the three basic operations: parietal cell vagotomy,
also called highly selective vagotomy (HSV) or proximal gastric
vagotomy, vagotomy and drainage (V+D), and vagotomy and distal
gastrectomy.
69.
• HSV seversthe vagal nerve supply to the proximal twothirds of the
stomach, where essentially all the parietal cells are located, and
preserves the vagal innervation to the antrum and pylorus and the
remaining abdominal viscera.
• Thus, the operation decreases total gastric acid secretion by about
75%, and GI side effects are rare.
71.
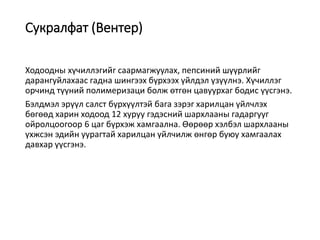
• Truncal vagotomyand pyloroplasty, and truncal vagotomy and
gastrojejunostomy are the paradigmatic vagotomy and drainage
procedures. HSV may be substituted for truncal vagotomy. The
advantage of V + D is that it can be performed safely and quickly by
the experienced surgeon.
• Truncal vagotomy denervates the antropyloric mechanism, and
therefore, some sort of procedure is necessary to ablate or bypass
the pylorus.
73.
• Gastrojejunostomy isa good choice in patients with gastric outlet
obstruction or a severely diseased proximal duodenum. The
anastomosis is done between the proximal jejunum and the most
dependent portion of the greater gastric curvature, in either an
antecolic or retrocolic fashion.
• Marginal ulceration is a potential complication. Mechanical
complications are also possible such as afferent or efferent loop
obstruction, internal hernia, and intussusception.
75.
• Pyloroplasty isuseful in patients who require a pyloroduodenotomy
to deal with the ulcer complication (e.g., posterior bleeding duodenal
ulcer), in those with limited or focal scarring in the pyloric region, or
when gastrojejunostomy is technically difficult.
• The most commonly performed pyloroplasty is the Heineke-Mikulicz
type (Fig. 26-36).
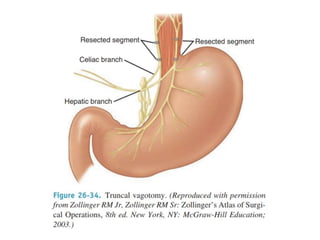
• Other occasionally useful techniques include the Finney (Fig. 26-37)
and the Jaboulay pyloroplasties (Fig. 26-38). These more extensive
pyloroplasty techniques may make subsequent distal gastric
resection more difficult and/or hazardous.
79.
• Although vagotomyand antrectomy (V + A) is associated with a very
low ulcer recurrence rate and is applicable to many patients with
complicated PUD (e.g., bleeding duodenal and gastric ulcer,
obstructing peptic ulcer, nonhealing gastric ulcer, and recurrent
ulcer), V + A has a higher operative mortality risk (compared with
HSV or V + D), and is irreversible.
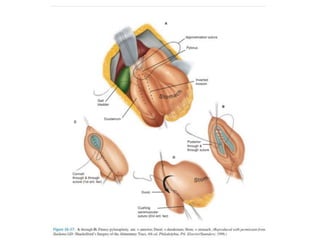
• Following antrectomy, GI continuity may be reestablished with a
Billroth I gastroduodenostomy (Fig. 26-39) or a Billroth II loop
gastrojejunostomy (Fig. 26-40).
82.
• Since antrectomyroutinely leaves a 60% to 70% gastric remnant,
routine reconstruction as a Roux-en-Y gastrojejunostomy should be
avoided (Fig. 26-41).
• Although the Roux-en-Y operation is an excellent procedure for
keeping duodenal contents out of the stomach and esophagus, in the
presence of a large gastric remnant, this reconstruction will
predispose to marginal ulceration and/or gastric stasis.
Hemorrhage
• Upper GIbleeding is a relatively common problem, with an annual
incidence of approximately 1 per 1000.
• Most nonvariceal bleeding (70%) is attributable to peptic ulcers.
• Several clinical scores have been created to risk-stratify
patients presenting with upper GI bleeding to predict risk of
rebleeding and overall morbidity and mortality. The most commonly
used scores are the Blatchford and Rockall prediction
scores.
89.
Hemorrhage
• The mostcommonly used system for classifying the endoscopic
appearance of bleeding ulcers is the Forrest classification (Table
48-4), which stratifies the risk of rebleeding based on observed
“stigmata of recent hemorrhage.”
• Guidelines for endoscopic control of bleeding published in
2010 advocate either the use of epinephrine plus an additional
method or monotherapy with either thermocoagulation or clipping,
but discourage the use of epinephrine alone.
92.
Hemorrhage
• All high-riskpatients should be placed in a monitored setting,
preferably an intensive care unit, until all bleeding has stopped for 24
hours. As part of the 2010 consensus guidelines, all highrisk
patients should be placed on a PPI administered intravenously,
with an initial bolus followed by continuous infusion or
intermittent dosing for up to 72 hours.
• Although flexible upper endoscopy remains the standard firstline
therapy for upper GI bleeding, another option for nonsurgical
control of bleeding duodenal ulcers is catheter-directed angiography
and endovascular embolization (Fig. 48-10).
95.
Perforation
• Patients withperforation typically complain of sudden-onset,
frequently severe epigastric pain. For many, it is their first symptom
of ulcer disease.
• Perforation has the highest mortality rate of any complication of
ulcer disease, approaching 15%.
• The perforation is usually in the first portion of the duodenum and
can easily be accessed through an upper midline incision.
• Perforations smaller than 1 cm can generally be closed primarily and
buttressed with a well vascularized omentum. For larger perforations
or ulcers with fibrotic edges that cannot be brought together without
tension, a Graham patch repair with a tongue of healthy omentum is
performed.
98.
Gastric outlet obstruction
•Acute inflammation of the duodenum can lead to mechanical
obstruction, with a functional gastric outlet obstruction manifested
by delayed gastric emptying, anorexia, nausea, and vomiting.
• Chronic inflammation of the duodenum may lead to recurrent
episodes of healing followed by repair and scarring, ultimately
leading to fibrosis and stenosis of the duodenal lumen.
• The standard operation for obstructing PUD is vagotomy and
antrectomy. Alternatively, vagotomy and gastrojejunostomy should
be considered if a difficult duodenal stump is anticipated with
resection.
• HSV and gastrojejunostomy may be comparable to V + A for
obstructing ulcer disease,124 and this procedure is appealing
because it can be done laparoscopically and does not complicate
future resection, if needed. However, potentially curable gastric or
duodenal cancers can be missed with this approach.
99.
Intractable or NonhealingPeptic Ulcer
• Surgical treatment should be considered in patients with nonhealing
or intractable PUD who have multiple recurrences, large ulcers (>2
cm), complications (obstruction, perforation, or hemorrhage), or
suspected malignancy. Definitive operation, particularly gastric
resection, should be considered most cautiously in the thin or
marginally nourished individual.
• If surgery is necessary, a lesser operation may be preferable. It is
prudent to avoid truncal vagotomy and/or distal gastrectomy as the
initial elective operation for intractable peptic ulcer in the thin or
asthenic patient.
100.
• Alternatives forintractable duodenal ulcer include HSV with or
without gastrojejunostomy (reversible drainage operation).
• In patients with nonhealing gastric ulcer, wedge resection with HSV
should be considered in thin or frail patients. Otherwise, distal
gastrectomy (to include the ulcer) is recommended.
• It is unnecessary to add a vagotomy in patients with type I or type IV
(juxta-esophageal) gastric ulcers because they are usually associated
with acid hyposecretion. Type IV gastric ulcers may be difficult to
resect as part of a distal gastrectomy, and a variety of surgical
techniques have been described to treat these more proximal lesions
(Fig. 26-45).