SPLEEN
• Spleen isreticuloendothelial organ ,that has its embryologic origin in
dorsal mesogastrium about 5weeks gestation .
• Adult location :in left upper quadrant attached to stomach via
gastrolineal ligament and to kidney by lienorenal ligament.
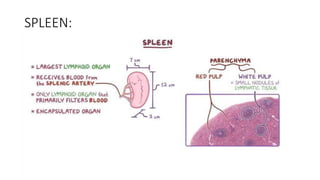
• It is largest lymphoid organ.
• It is encapsulated organ.
3.
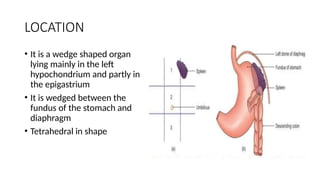
LOCATION
• It isa wedge shaped organ
lying mainly in the left
hypochondrium and partly in
the epigastrium
• It is wedged between the
fundus of the stomach and
diaphragm
• Tetrahedral in shape
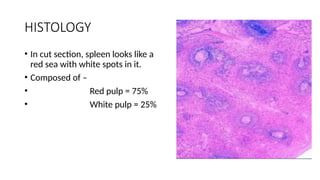
HISTOLOGY
• In cutsection, spleen looks like a
red sea with white spots in it.
• Composed of –
• Red pulp = 75%
• White pulp = 25%
6.
RED PULP
• Thered pulp is primarily involved in:
• • Filtering the blood
• • Recycling old or damaged red blood cells (RBCs)
• • Storing platelets
• • Acting as a blood reservoir (in some animals)
7.
RED PULP
• Thered pulp consists of:
• 1. Splenic Sinusoids:
• • Blood-filled channels lined by specialized endothelial cells (stave
cells).
• • These sinusoids allow selective passage of healthy blood cells,
while old or damaged ones are trapped.
• 2. Splenic Cords (Cords of Billroth):
• • Located between sinusoids.
• • Made of reticular connective tissue rich in macrophages,
monocytes, plasma cells, and blood cells (RBCs, platelets, etc.).
• • Macrophages here phagocytose old or abnormal RBCs and
pathogens.
8.
WHITE PULP
• Composedof lymphoid tissue (similar to lymph nodes).
• • Involved in the production and activation of lymphocytes
(especially B and T cells).
• • Acts like a filter for pathogens in the blood.
9.
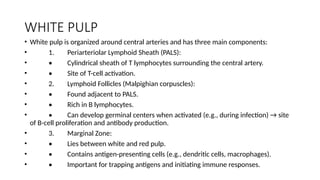
WHITE PULP
• Whitepulp is organized around central arteries and has three main components:
• 1. Periarteriolar Lymphoid Sheath (PALS):
• • Cylindrical sheath of T lymphocytes surrounding the central artery.
• • Site of T-cell activation.
• 2. Lymphoid Follicles (Malpighian corpuscles):
• • Found adjacent to PALS.
• • Rich in B lymphocytes.
• • Can develop germinal centers when activated (e.g., during infection) → site
of B-cell proliferation and antibody production.
• 3. Marginal Zone:
• • Lies between white and red pulp.
• • Contains antigen-presenting cells (e.g., dendritic cells, macrophages).
• • Important for trapping antigens and initiating immune responses.
10.
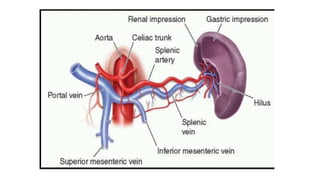
BLOOD SUPPLY
• Bloodsupply : SPLENIC ARTERY
• Venous drainage : SPLENIC VEIN
• Nerve supply : It has only sympathetic supply(Vasomotor)
• Lymphatic supply : via SUBCAPSULAR LYMPHATIC PLEXUS into
SPLENIC HILAR LYMPH NODES and finally into CELIAC NODES
12.
FUNCTIONS
• Maintanence ofquality control over erythrocytes in red pulp by
removal of senescent and defective red blood cells.
• Synthesis of antibodies in white pulp.
• Removal of antibody coated bacteria and antibody coated blood cells
from circulation.
• Spleen is in portal circulation.
• Blood flows into spleen at rate of 150ml/min through splenic
artery ,ultimately ramifies into central arterioles.
• Some blood goes from arterioles to capillaries and then to splenic
veins and out of spleen.
13.
• Majority ofthe blood from central arterioles flows into macrophages
lined sinuses and cords.
• Blood entering sinuses reenters the circulation through the splenic
venules.
• To return to circulation ,blood cells in cords must squeeze through
slits in cord lining to enter the sinuses that lead to venules.
• Old and damaged erythrocytes are less deformable and are retained
in cords ,where they are destroyed and their components recycled.
15.
• Red cellinclusions such as parasites,nuclear residua(Howell-jolly
bodies) or denatured hemoglobin( Heinz bodies) are pinched off in
process of passing through the slits a process called Pitting.
• Culling of dead and damaged cells and pitting of cells with inclusions
appear to occur without delay .
• Because the blood transit time through the spleen is only slightly
slower than in other organs.
16.
ADAPTIVE FUNCTIONS OFSPLEEN:
• 1)Clearance of bacteria and particulates from blood.
• 2)Generation of immune responses to certain pathogens.
• 3)Generation of cellular components of blood (extramedullary
hematopoiesis)
• Normal human Spleen contains approximately 1/3rd
of the total body
platelets and significant number of marginated neutrophils.
17.
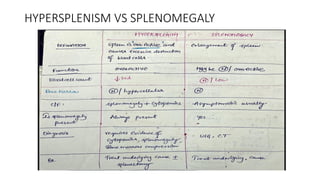
APPROACH TO SPLENOMEGALY:
•Heavy sensation in LUQ.
• Massive splenomegaly causes early satiety.
• Pain may result in acute swelling of spleen with stretching of capsule.
• SUBACUTE BACTERILA ENDOCARDITIS can present with severe LUQ
and pleuritic chest pain may accompany thromboembolic occlusion of
splenic blood flow.
18.
• PALPABLE SPLEENis major physical sign suggesting enlargement of
spleen.
• Normal spleen1) weighs <250 gms
• 2)decreases in size with age
• 3)lies within rib cage,
• 4)maximum cephalocaudal diameter of13cm by USG
20.
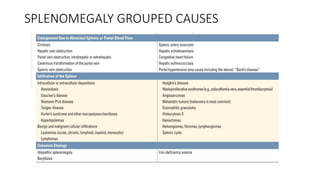
SPLENOMEGALY:
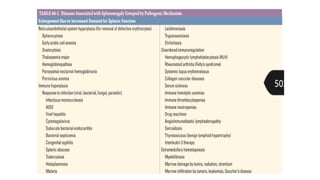
• 1)Enlargement dueto increased demand for splenic function.
• 2)Enlargement due to abnormal splenic or portal blood flow.
• 3)Infiltration of spleen.
• 4)Infiltration.
21.
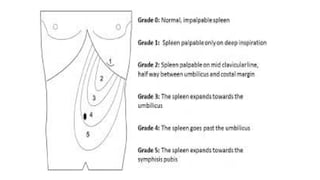
CLASSIFICATION OF SPLENOMEGALY
•Mild - Spleen palpable but not extending below the umbilicus
• Moderate - Extends below the umbilicus but not to pelvis
• Massive - Extends into pelvis or across midline
TROPICAL SPLENOMEGALY
• Alsoknown as HYPER REACTIVE MALARIAL SPLENOMEGALY.
• One of the leading causes of splenomegaly in malaria endemic areas.
• PATHOLOGY:
• 1) Aberrant immune response to chronic antigenic
stimulationexcessive production of immunoglobulins especially of
IgM TYPEthese Ig aggregate to form macroglobulins i.e high
molecular weight immune complexes.
26.
DIAGNOSTIC CRITERIA:
• MAJORCRITERIA:
• 1)Persistent gross splenomegaly extending more than 10 cm below
costal margin without any apparent cause.
• 2)Elevated anti malarial antibody titre ,IGM>2SD above the mean
value
• 3)Favourable response to long term malaria prophylaxis.
27.
MINOR CRITERIA:
• Hepaticsinusoidal lymphocytosis.
• normal cellular or humoral response to other antigenic stimulus
• Hypersplenism
• Lymphocyte proliferation
• occurrence in family and tribes.
28.
CLINICAL FEATURES
• Abdominalswelling
• Dragging sensation in abdomen
• Acute left sided abd pain secondary to splenic infarction.
• Increased susceptibility to infections
• Bleeding manifestations
• ON PHYSICAL EXAMINATIONmassive splenomegaly often extending
across the midline to right side of abdomen or downward into RIF
29.
LAB FINDINGS
• Pancytopeniaespecially anemia.
• Reticulocytosis.
• Thin and thick smear examined under geimsa stain.
• Increased bilirubin
• Sinusoidal lymphocytosis on liver biopsy.
30.
MANAGEMENT
• Enlarged spleenregresses over period of months with effective
antimalarial prophylaxis.
• Drugs like chloroquine,mefloquine.
• FOLLOWING ARE NOT INDICATED:
• Splenectomy
• Splenic irradiation
• Antimitotic therapy
31.
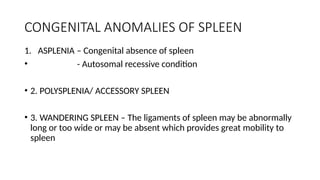
CONGENITAL ANOMALIES OFSPLEEN
1. ASPLENIA – Congenital absence of spleen
• - Autosomal recessive condition
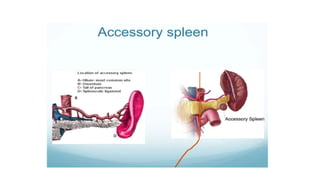
• 2. POLYSPLENIA/ ACCESSORY SPLEEN
• 3. WANDERING SPLEEN – The ligaments of spleen may be abnormally
long or too wide or may be absent which provides great mobility to
spleen








































![medical disorders complicating pregnancy 2[1] [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/medicaldisorderscomplicatingpregnancy21autosaved-241125191223-0fc12df0-thumbnail.jpg?width=640&height=640&fit=bounds)



















