Downloaded 38 times


![EFFICACY POLARIS-1
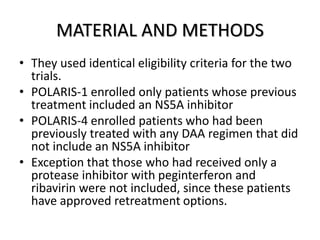
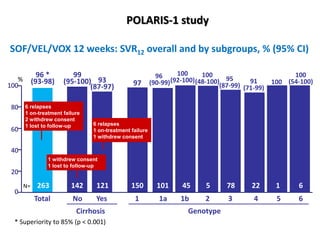
• The overall rate of SVR in the sofosbuvir–velpatasvir–
voxilaprevir group was 96% (95% confidence interval
[CI], 93 to 98), which was significantly superior to the
pre specified performance goal of 85% (P<0.001)
• Of the 253 patients with SVR 12 week after treatment,
i. 249 returned for the post-treatment week 24 visit.
ii. All 249 patients had a SVR at that time.
• None of the patients who received placebo had a SVR.](https://image.slidesharecdn.com/sofosbuvirppt-170906160043/85/Sofosbuvir-ppt-30-320.jpg)
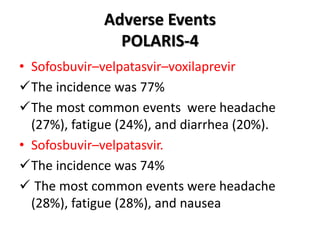



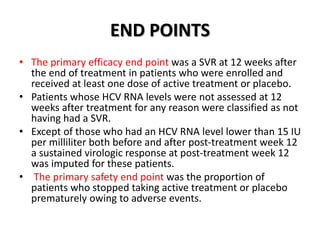
The document summarizes results from two phase 3 clinical trials that assessed the efficacy and safety of a fixed-dose combination of sofosbuvir, velpatasvir, and voxilaprevir for 12 weeks in patients with hepatitis C virus (HCV) who had previously received unsuccessful treatment with direct-acting antiviral (DAA)-based regimens. In POLARIS-1, the overall sustained virologic response rate was 96% among those receiving sofosbuvir, velpatasvir, and voxilaprevir, significantly higher than the prespecified goal of 85%. In POLARIS-4, patients receiving sofosbuvir, velpatasvir, and voxilap


































![[2015] hcv direct acting antivirals [da as] stumbling](https://cdn.slidesharecdn.com/ss_thumbnails/2015hcvdirectactingantiviralsdaasstumbling-151117003903-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)























![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)





