Download to read offline
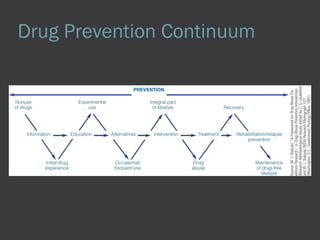

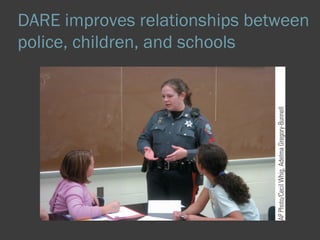

The document discusses approaches to drug prevention and education. It describes how most drug prevention funds in the US come from the federal government and are allocated to various agencies. Effective drug prevention programs are school-based, involve peers, emphasize social influences and life skills, aim to change social norms, and include parent and community involvement. While early efforts focused on supply reduction, the focus is now on prevention and underlying factors contributing to drug abuse. Successful programs provide skills training, social resistance training, and normative education in a culturally sensitive way over multiple years.























































![The Role of Education & Prevention in Reducing Prevalence of NPS [January 2016]](https://cdn.slidesharecdn.com/ss_thumbnails/mot-roleofeducationpreventioninreducingnps-jan2016-160120120907-thumbnail.jpg?width=640&height=640&fit=bounds)



























