
Recommended
Recommended
More Related Content
Similar to Skip to main contentiframe src=www.googletagmanager.comns.h.docx
Similar to Skip to main contentiframe src=www.googletagmanager.comns.h.docx (14)
More from jennifer822
More from jennifer822 (20)
Recently uploaded
Recently uploaded (20)
Skip to main contentiframe src=www.googletagmanager.comns.h.docx
- 1. Skip to main content <iframe src="//www.googletagmanager.com/ns.html?id=GTM- 5M58KS" height="0" width="0" style="display:none;visibility:hidden"></iframe> Top of Form Bottom of Form MENU Browse Resources Authors Librarians Editors Societies Advanced Search IN THIS JOURNAL Journal Home Browse Journal Current Issue OnlineFirst All Issues Submit Paper About More Information Editorial Board Free Sample Email Alerts Feedback Recommend to Library Advertise
- 2. Reprints RSS Subscribe Advanced Search Browse Resources Authors Librarians Editors Societies Advanced Search Top of Form Bottom of Form Advanced Sign In Apollo Group - UOP Society Access Options You can be signed in via any or all of the methods shown below at the same time. My Profile Sign in here to access free tools such as favourites and alerts, or to access personal subscriptions Top of Form Email (required) Password (required): Forgotten your password? Set new password
- 3. Remember me Bottom of Form I don't have a profile Create Profile I am signed in as: View My Account Logout With my free profile I can: Set up favourite journals and register for email alerts List saved searches Edit account details Activate personal subscriptions and access content Institution If you have access to journal content via a university, library or employer, sign in here Shibboleth Open Athens I am signed in via: Apollo Group - UOP Sign in via: Shibboleth Sign in via: Open Athens With institutional access I can: View or download all content the institution has subscribed to. Society If you have access to journal via a society or associations, read the instructions below Top of Form Members of _ can log in with their society credentials below Username (required) Password (required)
- 4. Society (required) Bottom of Form Access to society journal content varies across our titles. If you have access to a journal via a society or association membership, please browse to your society journal, select an article to view, and follow the instructions in this box. Contact us if you experience any difficulty logging in. Some society journals require you to create a personal profile, then activate your society account Activate my Society Account I am signed in via: Institution my society or association Logout With society access I can: View or download all the content the society has access to. Need Help? Contact SAGE Need Help? Contact SAGE American Journal of Health Promotion 1.957 Impact Factor Journal Indexing & Metrics » Journal Home Browse Journal Current Issue OnlineFirst All Issues Submit Paper About
- 5. More Information Editorial Board Free Sample Email Alerts Feedback Recommend to Library Advertise Reprints RSS Subscribe Top of Form Search in: Bottom of Form Add Email Alerts close Add Email Alerts Dialog You are adding the following journals to your email alerts Top of Form Journal New Content Announcements American Journal of Health Promotion Bottom of Form Contents Full Article Content List Abstract Introduction Methods Results Discussion Conclusions
- 6. Acknowledgments References Article Menu Download PDF Full Article Content List Abstract Introduction Methods Results Discussion Conclusions Acknowledgments References Figures & Tables Article Metrics Cite Citation Tools How to cite this article If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click on download. Top of Form How to cite this article Style
- 7. Copy to Clipboard Citation copied to clipboard. Format Tips on citation download Download Citation Bottom of Form Download article citation data for: Population-Level Measures to Predict Obesity Burden in Public Schools: Looking Upstream for Midstream Actions Wasantha P. Jayawardene, MD, PhD, David K. Lohrmann, PhD, Stephanie Dickinson, MAS, and Mohammad R. Torabi, PhD American Journal of Health Promotion201632:3, 708-717 Download Citation If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click on download. Top of Form Format Tips on citation download Download Citation Bottom of Form
- 8. Download article citation data for: Population-Level Measures to Predict Obesity Burden in Public Schools: Looking Upstream for Midstream Actions Wasantha P. Jayawardene, MD, PhD, David K. Lohrmann, PhD, Stephanie Dickinson, MAS, and Mohammad R. Torabi, PhD American Journal of Health Promotion201632:3, 708-717 Share Share Social Media Email Share Access double-click to add/edit rich text ... double-click to add/edit rich text ... All fields are required Top of Form Recipient's Email Address: Your Email: Your Name: Subject: Send me a copy Retype the code from the picture:
- 9. Cancel Bottom of Form Access sharing is not available double-click to add/edit rich text ... Accept terms and conditions Terms and conditions Copy to clipboard Via Social Media Via Email All fields are required Top of Form Recipient's Email Address: Your Email: Your Name: Subject: Send me a copy Cancel Bottom of Form Request Permissions View permissions information for this article View Related Articles
- 10. Comments Explore More Download PDF Population-Level Measures to Predict Obesity Burden in Public Schools: Looking Upstream for Midstream Actions Show all authors Wasantha P. Jayawardene, MD, PhD1 Wasantha P. Jayawardene 1Applied Health Science, School of Public Health Bloomington, Indiana University, Bloomington, IN, USA See all articles by this author Search Google Scholar for this author , David K. Lohrmann, PhD1 David K. Lohrmann 1Applied Health Science, School of Public Health Bloomington, Indiana University, Bloomington, IN, USA See all articles by this author Search Google Scholar for this author , Stephanie Dickinson, MAS2 Stephanie Dickinson 2Epidemiology and Biostatistics, School of Public Health Bloomington, Indiana University, Bloomington, IN, USA See all articles by this author Search Google Scholar for this author , Mohammad R. Torabi, PhD1 Mohammad R. Torabi 1Applied Health Science, School of Public Health Bloomington, Indiana University, Bloomington, IN, USA See all articles by this author Search Google Scholar for this author ... First Published October 5, 2016 Research Article https://doi- org.contentproxy.phoenix.edu/10.1177/0890117116670305
- 11. https://doi- org.contentproxy.phoenix.edu/10.1177/0890117116670305 Article information Article Information Volume: 32 issue: 3, page(s): 708-717 Article first published online: October 5, 2016; Issue published: March 1, 2018 Wasantha P. Jayawardene, MD, PhD1, David K. Lohrmann, PhD1, Stephanie Dickinson, MAS2, Mohammad R. Torabi, PhD1 1Applied Health Science, School of Public Health Bloomington, Indiana University, Bloomington, IN, USA 2Epidemiology and Biostatistics, School of Public Health Bloomington, Indiana University, Bloomington, IN, USA Corresponding Author: Wasantha P. Jayawardene, Applied Health Science, School of Public Health Bloomington, Indiana University, PH 116, 1025 E 7th Street, Bloomington, IN 47405, USA. Email: [email protected] Abstract Full Text References PDF Abstract Section: Top of Form Bottom of Form
- 12. Purpose: To estimate school-level obesity burden, as reflected in prevalence of obesity, based on the characteristics of students’ socioeconomic and geographic environments. Design: Secondary analysis of cross-sectional data. Setting: Public schools (N = 504) from 43 of 67 counties in Pennsylvania. Participants: Kindergarten through grade 12 students (N = 255 949). Measures: School-level obesity prevalence for the year 2014 was calculated from state-mandated student body mass index (BMI) measurements. Eighteen aggregate variables, characterizing schools and counties, were retrieved from federal data sources. Analysis: Three classification variables—excess weight (BMI ≥ 85th percentile), obesity (BMI ≥ 95th percentile), and severe obesity (BMI > 35% or 120% of 95th percentile)—each with 3 groups of schools (low-, average-, and high-prevalence) were created for discriminant function analysis, based on state mean and standard deviation of school distribution. Analysis tested each classification model to reveal school- and county-level dimensions on which school groups differed from each other. Results: Discriminant functions for obesity, which contained school enrollment, percentage of students receiving free/reduced-price lunch, percentage of black/Hispanic students, school location (suburban/other), percentage of county adults with postsecondary education, and percentage of county adults with obesity, yielded 67.86% correct classification (highest accuracy), compared to 34.23% schools classified by chance alone. Conclusion:
- 13. In the absence of mandated student BMI screenings, the model developed in this study can be used to identify schools most likely to have high obesity burden and, thereafter, determine dissemination of enhanced resources for the implementation of proven prevention policies and programs. Keywords demographic factors, socioeconomic factors, geographic factors, classification, schools, obesity Introduction Section: Top of Form Bottom of Form In 2012, 34.2% of US elementary school-aged children and 34.5% of secondary school-aged adolescents were overweight; respectively, 17.7% and 20.5% were obese.1 Obesity burden is experienced disproportionately across demographic subgroups and differs across communities, schools, and regions.2 Since African American race, Hispanic ethnicity, low household income, and parental education plus living in inner city are associated with overweight,3 schools in neighborhoods with higher proportions of such families likely have higher rates of child overweight and obesity.2 Ethnic disparities related to childhood obesity are widening with rates increasing faster among non-Hispanic black and Mexican American boys than non-Hispanic white boys, and among non-Hispanic black girls than non-Hispanic white girls.4 These social environment characteristics (ie, upstream determinants) influence behaviors and health status of children and families.5,6 Population-level obesity prevention includes multilevel school and child health policies (ie, upstream interventions), school- and community-based programs (ie, midstream interventions), and need-based individualized behavioral approaches (ie, downstream interventions).6 Schools are important settings for multicomponent preventive programs that improve weight status of children and adolescents by addressing attitudes and
- 14. behaviors related to physical inactivity, healthy dietary habits, and mental health.7 Prevention policy and program implementation varies,8 likely contributing to overweight and obesity prevalence differences across schools.9-11 In consideration of nationwide interventions, schools involved in on-site Healthy Schools Program demonstrated a trend toward decreased overweight (−0.48%) and obesity (−0.42%) with each additional contact with the program and each additional year of exposure.11 From a statewide perspective, students exposed to strong, specific, competitive food laws in 2003, compared to students in states with no such laws, gained 0.25 less body mass index (BMI) units on average from fifth to eighth grade and were less likely to remain overweight or obese; also, if laws remained consistently strong over a 3-year period, students gained 0.44 fewer BMI units compared to students in states with no such laws.10 In consideration of school-based interventions, healthier school environments led to 15.2% relative reduction in obesity prevalence among elementary school students over 6 years, while the number of obesity prevention strategies implemented was negatively associated with overweight and obesity prevalence over time.9 Therefore, student overweight and obesity variability among public schools are attributed to differences in health disparities across social environments (ie, upstream determinants) or school-based obesity prevention outcomes (ie, midstream interventions) or both. Contextually, BMI-based identification of children at greatest health risk due to excess body fat is essential. Prior studies found that the obesity prevalence is higher in states with school-based BMI surveillance mandates; although causality was not established, this is likely due to the circumstance that such states consider the obesity problem as more serious and, consequently, enact BMI-screening policies.12 Despite limitations, estimation of childhood obesity burden through school-based BMI measurement by trained personnel can identify high-risk groups, monitor progress toward achieving objectives, and foster policy and/or program changes.13 Such
- 15. initiatives provide specific obesity burden estimates used to inform design and implementation of school-level efforts; interventions should be responsive to the existing obesity burden within schools.14 Twenty states require BMI surveillance and 9 recommend periodic body composition or fitness screenings.12 However, even within states with BMI screening mandates, all schools do not consistently collect BMI data.13 Thus, development of a clearly articulated model of health disparities6 with rational links between social environments (ie, upstream determinants) and school-level BMI outcomes is warranted to allow better approximation of obesity burden within schools when BMI data are unavailable. Interventions that are funded and designed based on well- informed obesity burden estimates, accounting for empirically established links between health disparities and varying obesity rates across schools, can ultimately improve outcomes, cost- effectiveness, and community benefits. Purpose The objective of this study was to determine school-level obesity burden, based on the characteristics of the social, economic, and geographic environments of students. The research question was: “Can publicly available school-level and population-level variables predict school classification by student obesity prevalence?” Methods Section: Top of Form Bottom of Form Design The study involved a secondary analysis of cross-sectional data. Sample Multisource data from 43 of 67 Pennsylvania counties were accessed. Geographically, counties included 19 of the 20 most populous as well as all of Pennsylvania’s 10 largest cities. The
- 16. sample consisted of 504 public elementary and secondary schools that reported measured height and weight data of 255 949 students in grades K-12 for the year 2014. Measures Eighteen potential discriminating (predictor) variables were identified—9 at school level and 9 at county level. Public school characterization variables were total students, percentage of students eligible for free lunch (≤130% of federal poverty threshold), percentage of students eligible for reduced-price lunch (≤185% of federal poverty threshold), percentage of black students, percentage of Hispanic students, percentage of male, school-level (eg, elementary, middle, high), student/teacher ratio, and school location based on urban-centric locale codes (1 = city large, 2 = city midsize, 3 = city small, 4 = suburb large, 5 = suburb midsize, 6 = suburb small, 7 = town fringe, 8 = town distant, 9 = town remote, 10 = rural fringe, 11 = rural distant, and 12 = rural remote). County-related variables were county population, percentage of African American (black), percentage of Hispanic, percentage of adults with postsecondary education, county median household income, percentage of population with limited healthy foods access, percentage of single parent households, percentage of low-birth-weight live births, and percentage of obese adults. Table 1 indicates the data source for each discriminant variable retained in the final model.15-17 Table 1. Publicly Available Data Sources for the Discriminant Variables in the Final Model. Table 1. Publicly Available Data Sources for the Discriminant Variables in the Final Model. View larger version Excess weight, obesity, and severe obesity were considered classification (dependent) variables. Centers for Disease Control and Prevention (CDC)-developed growth charts for children and adolescents (2000 as the growth reference year for
- 17. calculation of percentiles) were used to classify BMIs.18 Obesity burden variables—percentage of excess weight students (≥85th percentile), percentage of obese students (≥95th percentile), and percentage of severely obese students (≥120% of the 95th percentile or BMI > 35 regardless of age)19,20— were derived from 2014 student height and weight measurements. State-mandated height and weight measurements were taken by qualified personnel (eg, school nurses), using established protocols,12 and entered into an electronic health record.21 Data were compiled in 3 repositories maintained by Population Health Innovations, LLC22 and supported by the Highmark Foundation for Pittsburgh and most Pennsylvania counties, Independent Blue Cross for Philadelphia and surrounding counties, and Blue Cross of Northeast Pennsylvania for northeastern counties. Nonpublicly available de-identified BMIs were accessed under a data sharing agreement. Data were collected and analyzed in 2015. Analysis Files were configured into a relational database and then aggregated into 3 levels: student, school, and county. Data were validated by eliminating unrealistic values for height (≥7 ft or ≤3 ft), weight (≥ 350 pounds or ≤ 50 pounds), and BMI (≥55 or ≤7). Outliers constituted 103 of 255 949 students (0.04%). For each variable, normal distribution of data was required to meet the assumptions of the main analysis, that is, discriminant function analysis. Therefore, if the distribution was skewed, square root transformation was initially performed. If skewness still remained, log transformation was performed. Closely related variables, that is, (1) percentage of free lunch eligible students and percentage of reduced-price eligible students, (2) percentage of black students and percentage of Hispanic students, and (3) percentage of African American (black) population and percentage of Hispanic population were combined. As some of the 12 locale codes had very few schools and little difference between urban and rural obesity rates was found, school location was transformed into 2 binary variables:
- 18. (1) urban (locale categories 1-6) versus rural (other categories) and (2) suburban (locale categories 4-6) versus not suburban (other categories). Three Philadelphia schools constituted multivariate outliers and were eliminated because their Mahalanobis distance was 22.46 or greater at P < .001; calculation of the Mahalanobis distance was based on the multidimensional generalization of 6 independent variables. Although the statistical method cannot identify the potential reason case by case, a school can become a multivariate outlier due to errors (eg, sampling, data collection, data entry) or legitimately by random chance (eg, large enrollment plus unusually high level of poverty and minority students). Discriminant function analysis23 was performed using SPSS version 22.024 and SAS version 9.425 statistical packages. Discriminant function analysis assumptions required that groups of schools be mutually exclusive and group sizes not grossly different.23 To meet this assumption, in each classification variable (mean − 0.5 standard deviation [SD]) and (mean + 0.5 SD)] were utilized as cutoffs to obtain 3 school groupings (ie, low-, average-, and high-prevalence schools). Analysis revealed the population-level dimensions (ie, school and county level) on which 3 levels of each classification variable (excess weight, obesity, and severe obesity) differed. Three classification variables were examined separately with discriminant function analysis. For each classification, the best combination of discriminating variables was determined based on pooled within-group correlations between discriminating variables, functions at group centroids, and classification results.23 Then, the best classification variable was determined based on percentage of correctly classified schools.23 Results Section: Top of Form Bottom of Form
- 19. For 43 counties, average prevalence of excess weight, obesity, and severe obesity was 36.00%, 18.85%, and 6.42%, respectively. For each retained school, percentage of excess weight, obese, and severely obese students were calculated; SDs of those distributions were 4.77%, 3.83%, and 1.74%, respectively. Ranges were 18.42% to 52.04%, 6.25% to 32.43%, and 0.00% to19.46%. Obesity-based classification, compared to excess-weight- and severe-obesity-based classifications, yielded the highest rate of correctly classified schools (67.86% correct classification vs 34.23% classified by chance alone; 33.63% improvement; Table 2). Cross validation was done by the leave- one-out method, where each school was classified by the functions derived from all schools other than that school. Cross validation of obesity-based classification revealed a 66.18% correct classification (31.95% improvement). Since classification accuracy was established as the criterion for selecting the classification variable, only results from the obesity-based classification are presented and discussed below. School- and county-level variable ranges proved wide (Table 3). Table 2. Classification of Schools Based on Excess Weight, Obesity, and Severe-Obesity Burdens.a,b Table 2. Classification of Schools Based on Excess Weight, Obesity, and Severe-Obesity Burdens.a,b View larger version Table 3. Population Characteristics (A) and Unadjusted Group Means for Discriminant Variables in the Obesity-Based Classification (B). Table 3. Population Characteristics (A) and Unadjusted Group Means for Discriminant Variables in the Obesity-Based Classification (B).
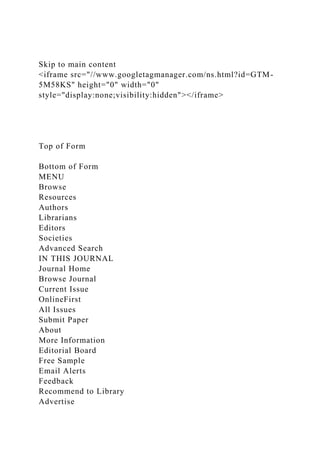
- 20. View larger version The final model for obesity-based classification, providing the highest discriminatory power with the least number of variables, contained 6 independent variables (5 continuous and 1 binary; Table 1): square root of total students (sq-#students), square root of percentage of free and reduced-price lunch eligible students (sq-poverty), logarithm of percentage of black and Hispanic students (log-minority), school’s location as suburban according to urban-centric locale codes (locale-suburb; 1 = suburban or 0 = urban or rural), percentage of county adults with some postsecondary education (adult-educ), and percentage of county adults who were obese (adult-obese). Sq-#students, sq-poverty, log-minority, locale-suburb, adult-educ, and adult- obese separated low-, average-, and high-obesity schools (P = .001 for sq-#students and P < .001 for other variables). At school level, log-minority positively correlated with sq-poverty (r = 0.598); other correlations were very weak (r < 0.25). At the county level, adult-educ negatively correlated with adult-obese (r = −0.742). Two discriminant functions were identified: sq-poverty (r = 0.922) alone was loaded on the first, whereas all other variables, that is log-minority (r = −0.690), adult-obese (r = 0.623), adult-educ (r = −0.536), locale-suburb (r = −0.474), and sq-#students (r = 0.332), were loaded on the second. The first function (rc = 0.709), based on the percentage of free and reduced-price lunch eligible students, maximally separated low- obesity schools from the rest, while also separating high-obesity schools from average-obesity schools to some extent (Figure 1). The second function (rc = 0.207), based on black/Hispanic percentage, adult obesity, adult education level, school location (ie, suburban or not), and school size, maximally separated average-obesity schools from the rest. Download Open in new tab Download in PowerPoint
- 21. Figure 1. Group centroids for unstandardized canonical discriminant functions: Function 1 = student poverty. Function 2 = adult education level, and school location (suburban or not), percentage of black/Hispanic, school size, and adult obesity. The canonical score plot demonstrates how the function 1 (x axis) and function 2 (y axis) classify schools between low-, average-, and high-obesity groups by plotting the observation score, computed via unstandardized canonical discriminant functions. Theoretically, each school is represented by a dot on the plot (476 dots in total); included in the graph are only the group centroid for low-, average-, and high-obesity groups. The first function (rc = 0.709), based on student poverty, maximally separated low-obesity schools from the rest, while it also separated high-obesity schools from average-obesity schools to some extent. The second function (rc = 0.207), based on black/Hispanic percentage, adult obesity, adult education level, school location (ie, suburban or not), and school size, maximally separated average-obesity schools from the rest. Standardized canonical discriminant function coefficients were estimated to standardize the distribution of scores from each function, utilizing a mean of 0 and SD of 1. The absolute value of these coefficients indicated the relative contribution of discriminating variables to function 1 and function 2. In function 1, greatest contribution was from sq-poverty (1.066), followed by adult-educ (−0.269), log-minority (−0.259), adult- obese (−0.156), and locale-suburb (−0.116), while the least important predictor was sq-#students (−0.004). In function 2, greatest contribution was from log-minority (−0.684), followed by sq-#students (0.549), adult-obese (0.499), locale-suburb (−0.347), and adult-educ (0.182), while the least important predictor was sq-poverty (0.122). Based on unadjusted group means (Table 3), low-obesity schools had highest student enrollment, least poverty, least percentage of black/Hispanic students, and were more likely to be in suburban counties with high rates of postsecondary
- 22. education and lower rates of adult obesity. The antithetical situation was observed for high-obesity schools; that is, the lowest student enrollment, highest poverty, highest percentage of black/Hispanic students, lowest percentage of suburban schools, lowest adult postsecondary education rate, and highest adult obesity rate. Using classification function coefficients, an equation was developed for each of the low- average-, and high-obesity groups to determine school assignment to group, based on the scores for 6 variables (Table 4). To improve correct classification, utilizing school- and county-level discriminant variables, a school should be assigned to the group for which it obtained the highest classification score; for example, if a rural school (locale-suburb = 0) has 225 students (sq-students = 15), with 49% free and reduced-price lunch eligibility (sq-poverty = 0.7), and 11% black and Hispanic students (log-minority = −0.9586), and is located in a county that has 23% of adults with postsecondary education (adult-educ = 0.23) and 38% of adults who are obese (adult-obese = 0.38), the school will score 298 for low obesity, 309 for average obesity, and 317 for high obesity; hence, the school will be assigned to the high-obesity group. Table 4. School Assignment to Obesity Burden Group, Based on Classification Function Coefficients.a Table 4. School Assignment to Obesity Burden Group, Based on Classification Function Coefficients.a View larger version Discussion Section: Top of Form Bottom of Form
- 23. Study results clearly demonstrate that publicly available school- level and county-level variables can be used to predict school classification by student obesity prevalence; resultant models included a rational combination of publicly available, population-level variables for classification of schools based on obesity burden, which, in comparison with classification by chance alone, almost doubled the percentage of correctly classified schools. Critical variables for determining high- obesity schools were common: lower student numbers, higher student poverty, higher minority student enrollment, nonsuburban location plus location in communities with lower adult education, and higher adult obesity levels. Results demonstrate that reliance on a single variable (eg, percentage of free and reduced-price lunch) is unlikely to provide the best approach to identifying schools in need of more robust interventions, because obesity burden clearly depends on multiple upstream health determinants (eg, race/ethnicity, poverty, and urban/rural divide), along with interactions that may also contribute to this variation (eg, rural poverty). Nevertheless, free or reduced-price lunch eligibility played a substantial role in classifying schools. Differentiation of low-, average-, and high-obesity schools involved a relatively stronger effect of poverty, compared to the effect of all other variables combined. This finding was unsurprising since previous studies confirmed that poverty leads to inequities in multiple factors (eg, quality housing, access to healthy food, access to quality education, and safe places to be physically active) that contribute to community obesity rates.26 According to 1999 to 2004 National Health and Nutrition Examination Survey (NHANES), 23% of 15- to 17-year-olds living in poverty were obese, compared to 14% obesity rate among adolescents not living in poverty.27 However, national data from 1971 to 2002 revealed a weakening association between poverty and childhood obesity over decades, especially among adolescents.28 This study’s finding that the percentage of black and Hispanic
- 24. students significantly predicted school obesity rates is supported by research which found that overweight and obesity rates are higher among black than white children.29 Furthermore, minority children’s obesity rates are increasing faster at earlier ages; by age 6 to 11, 26.1% of Hispanic children and 23.8% of African American children were obese compared with 13.1% of white children.29 Almost three- quarters of the difference in rates between Hispanic and white children occurs by third grade; three-quarters of the difference between African American and white children occurs between grades 3 and 8.30 Regarding upstream race/ethnicity-related determinants, almost one-fourth of Hispanic and black families had limited healthy food access due to lack of financial or other resources, versus 11% of white families.31 Fewer black (11.3%) and Hispanic (9.3%) than white adolescents (4.5%) eat vegetables during the prior week.32 Compared to predominantly white neighborhoods, outdoor advertising for unhealthy foods was 13 times greater in predominantly black neighborhoods and 9 times greater in predominantly Hispanic neighborhoods.33,34 Access to safe and quality public parks, green space, and sidewalks for physical activities was much lower in predominantly black and Hispanic neighborhoods.35 Substandard neighborhood safety had a strong negative impact on the amount of outdoor play by black girls36; Hispanic children engaged in less after-school physical activity due to cost and language barriers.37 Although poverty and obesity rates were higher among black and Hispanic families than white families, black race and Hispanic ethnicity are unlikely to be the sole reasons that track poverty; for example, 2005 to 2008 NHANES data revealed a significant inverse association of family income with obesity for white children but an inconsistent relationship for minority children.38 Contrary to expectations, a 1999 to 2004 NHANES study found higher obesity rates with higher family income among school-aged black children, especially girls.39 In 2005 to 2008, a similar but nonsignificant association was observed
- 25. for Mexican American girls. Put differently, most obese children do not live in poverty; 62% of 12 million US obese children are not impoverished. Just 27% of 6 million obese white children are impoverished.38 Although the urban-to-rural gradient and urban–rural binary variable did not improve classification of schools in the current study, use of a binary variable that categorized suburban schools versus all other schools significantly improved classification. Previous studies representing 8 states revealed that childhood obesity rates were highest in rural areas.40 Rural areas have the lowest food location availability, least nutrition education resources, and worst exercise facilities, while rural residents, on average, have lower incomes, lower education levels, and limited prevention and treatment options, all contributing to obesity.41 Meanwhile, many urban children also lack access to safe parks, playgrounds, and healthy foods and are more exposed to unhealthy foods; income modifies the relationship between food environment and BMI.42 The current study also demonstrated that the percentage of adults with some postsecondary education, even if measured at county level, can contribute to obesity-based school classifications. Empirical evidence suggested that the household head’s education level had a significant negative relationship to obesity prevalence, although not consistent across genders and race/ethnicity groups.38 Compared to 21.1% and 20.4% obesity prevalence among boys and girls, respectively, living in households where the head had no high school diploma, 11.8% and 8.3% obesity rates were found among boys and girls, respectively, who lived in households where the head had a college degree. The relationship between household head’s education and children’s obesity was statistically significant for both white and black girls. From 1988 to 2008, with the exception of girls living in homes where the head had a college degree, obesity prevalence of girls increased significantly at all levels of household head’s education.38 Finally, several family- and community-characteristics associated with poverty and
- 26. adult education potentially contribute to childhood obesity, for example dietary practices, screen time, parental behaviors and attitudes, home environment, and neighborhood physical activity opportunities.43 These may be addressed through specific obesity prevention interventions within a multilayered ecological context,43-45 although poverty reduction and adult education require broader and more upstream interventions. In addition to upstream determinants, school characteristics may contribute to obesity prevalence. The current study revealed that, although school type (ie, elementary, middle, or high) did not improve classification of schools for obesity, school enrollment size did. Number of students in school constitutes a proxy measure of both school type and urban–rural divide combined. Elementary schools usually have the least number of students, while high schools have the greatest numbers46; accordingly, elementary schools are more likely to be classified as high obesity; this supports the need for interventions during the earliest formative years. Also, rural schools are more likely to be classified as high obesity because they generally have fewer students than urban and suburban schools. Compared to all US schools in 2010, average student enrollment in Pennsylvania elementary schools was lower, while the averages for middle, high, and other (eg, junior high) schools were much higher, creating a wide range of within-state school sizes.46 Small schools in rural areas face unique challenges, including smaller food service programs, teacher shortages, and limited financial resources,47 although, compared to large schools, availability and purchase of competitive food and beverages by students in small schools may be favorable.48 While school program variables were not considered in this study, previous studies suggest that such midstream actions somewhat correlate with upstream determinants included in this study.49 For example, schools with higher poverty rates, compared to others, allowed students to purchase unhealthful competitive foods significantly more often.50 Finally, the current study demonstrated that, in the absence of
- 27. up-to-date county-level childhood obesity prevalence data, adult obesity prevalence data can be used to help classify schools. Obesity, once established in childhood, tends to persist through adult life51 and prevailing environmental conditions and behaviors conducive to weight gain in childhood usually operate in adult life. Thus, states and counties with relatively higher rates of adult obesity also tend to have higher rates of childhood obesity. Limitations This study has several limitations. Prior research revealed that children with excess body fat can be identified reasonably well using BMI criteria.52 However, interpretation of overweight (≥85th percentile but <95th percentile) in children utilizing age- sex-based BMI alone may not be fully accurate because some individuals, especially male adolescents, can be categorized as overweight due to high lean body mass rather than having excess fat.53 A similar misclassification is highly unlikely at ≥95th percentile, because assessment of body fat using standard methods (eg, dual-energy X-ray absorptiometry) revealed that almost all children identified as obese via BMI have excess body fat.54 From a study design perspective, not all public schools from each county provided student BMI, data were not available for all students in selected schools, and public schools were excluded from the analysis if demographic data were unavailable. Therefore, the possibility that systematic bias that occurred in school selection cannot be excluded. Height and weight data were collected for state-mandated health screenings, not for research purposes. Although height and weight measured by trained professionals, such as school nurses, are likely to be accurate, full-time nurses are unavailable in many schools.55 Additionally, many nurses believe that BMI surveillance is an added burden to their workload56; personnel assigned to assist nurses with BMI surveillance need technical training for measuring height and weight accurately.57,58 Electronic and beam balance scales used to accurately measure weight (spring balance scales are not
- 28. suitable) should be calibrated properly and regularly to the nearest one-fourth pound, following manufacturer’s directions, and stadiometers should measure height to the nearest one- eighth inch.58-60 Adherence to auxiliary personnel training and equipment quality-control standards for measuring student weight and height in all involved Pennsylvania schools cannot be fully guaranteed. Finally, although overall discriminant function classification accuracy was high, functions tended to overclassify low-obesity schools. Conclusions Section: Top of Form Bottom of Form Estimation of the obesity burden in schools utilizing publicly available school-level and community-level aggregate variables identified both the magnitude of the problem in a given school and related associations or childhood obesity risk factors. Thus, the models from this study can be used to (1) identify schools most likely to have high obesity levels, in the absence of routine student BMI screenings and (2) inform dissemination of enhanced resources for implementation of proven and robust prevention policies and programs. Public schools, clearly identified and supported by CDC as an integral part of the public health system,61,62 are expected to provide opportunities for students to adopt healthy lifestyles,63,64 regardless of socioeconomic status or ethnicity, even when communities and families are unable to do so. As mentioned in the introduction section, limited research have proven that school-based interventions (conducted at national, state, and local levels) were beneficial in reducing obesity rates. While reduction of student obesity rates is an added challenge for schools, especially high-poverty schools that struggle with meeting current academic standards, doing so is in schools’ best interest since children who were physically fit and ate healthily
- 29. had lower absenteeism, concentrated better on academic tasks, and received better grades, while childhood obesity was associated with several health and social problems that can negatively affect the academic performance.65 So What? Implications for Health Promotion Practitioners and Researchers What is already known on this topic? Empirical studies and body mass index (BMI) surveillance programs have confirmed the magnitude and health determinants of childhood obesity plus variations in childhood obesity burden across communities. What does this article add? This is the first study to estimate school-level obesity burden based on the characteristics of the socioeconomic and geographic environments in which students live and learn. What are the implications for health promotion practice and research? Even within those 20 states having BMI screening mandates, all schools do not consistently collect BMI data. Estimation of schools’ obesity burden utilizing publicly available school- and county-level aggregate variables identified both the magnitude of the problem in a given school and related associations and/or obesity determinants. Health promotion practitioners can utilize this unique information to allocate greater physical and human resources for implementation of prevention policies and programs in schools that likely have high obesity rates. Acknowledgments We thank Christina L. Wilds, DrPH, of Highmark Foundation and Robert G. Gillio, MD, of Population Health Innovations, LLC, for providing data from the Health eTools for Schools database and their support in the preparation of this article. We also thank Godfred Antwi for his contribution to data extraction from public-use databases. Declaration of Conflicting Interests The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this
- 30. article. Funding The author(s) received no financial support for the research, authorship, and/or publication of this article. References Section: Top of Form Bottom of Form 1. Ogden, CL, Carroll, MD, Kit, BK, Flegal, KM. Prevalence of childhood and adult obesity in the United States, 2011-2012. JAMA. 2014;311(8):806–814. Google Scholar | Crossref | Medline | ISI 2. Nanney, MS, Davey, C. Evaluating the distribution of school wellness policies and practices: a framework to capture equity among schools serving the most weight-vulnerable children. J Am Diet Assoc. 2008;108(9):1436–1439. Google Scholar | Crossref | Medline 3. US Department of Health and Human Services. The Surgeon General’s Call To Action To Prevent and Decrease Overweight and Obesity 2001. Rockville, MD: Office of the Surgeon General; 2001. Google Scholar 4. Fryar, CD, Carroll, MD, Ogden, CL. Prevalence of Overweight and Obesity Among Children and Adolescents: United States, 1963-1965 Through 2011-2012. Atlanta, GA: Division of Health and Nutrition Examination Surveys, Centers for Disease Control and Prevention; 2014.
- 31. Google Scholar 5. Satcher, D, Higginbotham, EJ. The public health approach to eliminating disparities in health. Am J Public Health. 2008;98(3):400–403. Google Scholar | Crossref | Medline | ISI 6. Gehlert, S, Sohmer, D, Sacks, T, Mininger, C, McClintock, M, Olopade, O. Targeting health disparities: a model linking upstream determinants to downstream interventions: knowing about the interaction of societal factors and disease can enable targeted interventions to reduce health disparities. Health Aff (Millwood). 2008;27(2):339–349. Google Scholar | Crossref | Medline | ISI 7. Khambalia, AZ, Dickinson, S, Hardy, LL, Gill, T, Baur, LA. A synthesis of existing systematic reviews and meta-analyses of school-based behavioural interventions for controlling and preventing obesity. Obes Rev. 2012;13(3):214–233. Google Scholar | Crossref | Medline | ISI 8. Brown, T, Summerbell, C. Systematic review of school-based interventions that focus on changing dietary intake and physical activity levels to prevent childhood obesity: an update to the obesity guidance produced by the National Institute for Health and Clinical Excellence. Obes Rev. 2009;10(1):110–141. Google Scholar | Crossref | Medline | ISI 9. Heelan, KA, Bartee, RT, Nihiser, A, Sherry, B. Healthier school environment leads to decreases in childhood obesity: the Kearney Nebraska story. Child Obes. 2015;11(5):600–607.
- 32. Google Scholar | Crossref | Medline | ISI 10. Taber, DR, Chriqui, JF, Perna, FM, Powell, LM, Chaloupka, FJ. Weight status among adolescents in states that govern competitive food nutrition content. Pediatrics. 2012;130(3):437–444. Google Scholar | Crossref | Medline | ISI 11. Madsen, KA, Cotterman, C, Crawford, P, Stevelos, J, Archibald, A. Effect of the Healthy Schools Program on prevalence of overweight and obesity in California schools, 2006-2012. Prev Chronic Dis. 2015;12:E77. Published May 21, 2015. Google Scholar | Crossref | Medline | ISI 12. Linchey, J, Madsen, KA. State requirements and recommendations for school-based screenings for body mass index or body composition, 2010. Prev Chronic Dis. 2011;8(5):A101. Google Scholar | Medline | ISI 13. Dietz, WH, Story, MT, Leviton, LC. Issues and implications of screening, surveillance, and reporting of children’s BMI. Pediatrics. 2009;124(suppl 1):S98–S101. Google Scholar | Crossref | Medline | ISI 14. American Heart Association . Policy Position Statement on Body Mass Index (BMI) Surveillance and Assessment in Schools. Washington, DC: American Heart Association; 2008. Google Scholar 15.
- 33. U.S. Department of Education, Institute of Education Sciences, National Center for Education Statistics. Search for Public Schools . 2015; CCD Public school data 2013-2014, 2014-2015 school years. http://nces.ed.gov/ccd/schoolsearch/. Accessed October 29, 2015. Google Scholar 16. U.S. Department of Agriculture , Economic Research Service. County-Level Data Sets. 2015. http://www.ers.usda.gov/data- products/county-level-data-sets/education.aspx. Accessed November 14, 2015. Updated April 04, 2016. Google Scholar 17. Chronic Disease Prevention and Health Promotion DoDT . County-Level Data. 2015. http://www.cdc.gov/diabetes/atlas/countydata/atlas.html. Updated May 7, 2014. Accessed October 10, 2015. Google Scholar 18. Centers for Disease Control and Prevention NCfHS . CDC Growth Charts: United States. 2000. http://www.cdc.gov/growthcharts/. Updated September 9, 2010. Accessed July 21, 2011. Google Scholar 19. Kelly, AS, Barlow, SE, Rao, G. Severe obesity in children and adolescents: identification, associated health risks, and treatment approaches: a scientific statement from the American Heart Association. Circulation. 2013;128(15):1689–1712. Google Scholar | Crossref | Medline | ISI 20.
- 34. Ogden, CL, Carroll, MD, Curtin, LR, Lamb, MM, Flegal, KM. Prevalence of high body mass index in US children and adolescents, 2007-2008. JAMA. 2010;303(3):242–249. Google Scholar | Crossref | Medline | ISI 21. Lohrmann, D, YoussefAgha, A, Jayawardene, W. Trends in body mass index and prevalence of extreme high obesity among Pennsylvania children and adolescents, 2007–2011: promising but cautionary. Am J Public Health. 2014;104(4):e62–e68. Google Scholar | Crossref | Medline | ISI 22. Gillio, R. Population Health Innovations, Inc: Health eTools Platform. 2015. http://www.populationhealthinnovations.com/. Accessed January 02, 2016. Google Scholar 23. Tabachnick, BG, Fidell, LS. Using Multivariate Statistics. 6th ed. Boston, MA: Allyn and Bacon; 2013. Google Scholar 24. IBM SPSS Statistics for Windows [computer program]. Version 22.0. Armonk, NY: IBM Corp; 2012. Google Scholar 25. Base SAS® 9.4 Procedures Guide [computer program]. Cary, NC: SAS Institute Inc; 2015. Google Scholar 26. Singh, GK, Siahpush, M, Kogan, MD. Rising social inequalities in US childhood obesity, 2003-2007. Ann Epidemiol.
- 35. 2010;20(1):40–52. Google Scholar | Crossref | Medline | ISI 27. Miech, RA, Kumanyika, SK, Stettler, N, Link, BG, Phelan, JC, Chang, VW. Trends in the association of poverty with overweight among US adolescents, 1971-2004. JAMA. 2006;295(20):2385–2393. Google Scholar | Crossref | Medline | ISI 28. Wang, Y, Zhang, Q. Are American children and adolescents of low socioeconomic status at increased risk of obesity? Changes in the association between overweight and family income between 1971 and 2002. Am J Clin Nutr. 2006;84(4):707–716. Google Scholar | Crossref | Medline | ISI 29. Skinner, A, Skelton, JA. Prevalence and trends in obesity and severe obesity among children in the United States, 1999-2012. JAMA Pediatr. 2014;168(6):561–566. Google Scholar | Crossref | Medline | ISI 30. Rendall, MS, Weden, MM, Fernandes, M, Vaynman, I. Hispanic and black US children’s paths to high adolescent obesity prevalence. Pediatr Obes. 2012;7(6):423–435. Google Scholar | Crossref | Medline | ISI 31. Coleman-Jensen, A, Nord, M, Singh, AK. Household Food Security in the United States in 2012. Washington, D.C.: United States Department of Agriculture, Economic Research Service; 2013. Google Scholar
- 36. 32. Centers for Disease Control and Prevention . Youth Risk Behavior Survey, 2013. Atlanta, GA: Centers for Disease Control and Prevention; 2014. Google Scholar 33. Yancey, AK, Cole, BL, Brown, R. A cross-sectional prevalence study of ethnically targeted and general audience outdoor obesity-related advertising. Milbank Q. 2009;87(1):155–184. Google Scholar | Crossref | Medline | ISI 34. Robert Wood Johnson Foundation . Healthier Marketing and Latino Kids, Issue Brief. Princeton, NJ: Robert Wood Johnson Foundation; 2013. Google Scholar 35. National Recreation and Park Association . Parks and Recreation in Underserved Areas: A Public Health Perspective. Ashburn, VA: National Recreation and Park Association; 2013. Google Scholar 36. Dias, JJ, Whitaker, RC. Black mothers’ perceptions about urban neighborhood safety and outdoor play for their preadolescent daughters. J Health Care Poor Underserved. 2013;24(1):206– 219. Google Scholar | Crossref | Medline | ISI 37. London, R. After-School Fitness Programs Can Improve Children’s Health. San Antonio, TX: Robert Wood Johnson Foundation; 2013. Google Scholar
- 37. 38. Ogden, CL, Lamb, MM, Carroll, MD, Flegal, KM. Obesity and socioeconomic status in children: United States 1988–1994 and 2005–2008. NCHS data brief no 51. Hyattsville, MD: National Center for Health Statistics; 2010. Google Scholar 39. Freedman, DS, Ogden, CL, Flegal, KM, Khan, LK, Serdula, MK, Dietz, WH. Childhood overweight and family income. MedGenMed. 2007;9(2):26. Google Scholar | Medline 40. McMurray, RG, Harrell, JS, Bangdiwala, SI, Deng, SB. Cardiovascular disease risk factors and obesity of rural and urban elementary school children. J Rural Health. 1999;15(4):365–374. Google Scholar | Crossref | Medline | ISI 41. Liu, J, Bennett, KJ, Harun, N, Zheng, X, Probst, JC, Pate, RR. Overweight and Physical Inactivity among Rural Children Aged 10-17: A National and State Portrait. Columbia, SC: South Carolina Rural Health Research Center; 2007. Google Scholar 42. Shearer, C, Rainham, D, Blanchard, C, Dummer, T, Lyons, R, Kirk, S. Measuring food availability and accessibility among adolescents: Moving beyond the neighbourhood boundary. Soc Sci Med. 2015;133:322–330. Google Scholar | Crossref | Medline | ISI 43.
- 38. Kumanyika, S, Grier, S. targeting interventions for ethnic minority and low-income populations. Future Child. 2006;16(1):187–207. Google Scholar | Crossref | Medline | ISI 44. Khan, LK, Sobush, K, Keener, D. Recommended Community Strategies and Measurements to Prevent Obesity in the United States. Atlanta, GA: Division of Nutrition, Physical Activity, and Obesity, National Center for Chronic Disease Prevention and Health Promotion, CDC; 2009. Google Scholar 45. Institute of Medicine (IOM) . Preventing Childhood Obesity: Health in the Balance. Washington, DC: Institute of Medicine (IOM); 2005. Google Scholar 46. Chen, C, Sable, J, Mitchell, L. Documentation to the NCES Common Core of Data Public Elementary/ Secondary School Universe Survey: School Year 2009–10 (NCES 2011–348 rev). U.S. Department of Education. Washington, DC: National Center for Education Statistics; 2012. http://nces.ed.gov/pubsearch/pubs.info.asp?pubid=2011348rev. Accessed December 11, 2015. Google Scholar 47. Heneghan, AM, Malakoff, ME. Availability of school health services for young children. J Sch Health. 1997;67(8):327–332. Google Scholar | Crossref | Medline | ISI 48. Nollen, NL, Befort, C, Davis, AM. competitive foods in
- 39. schools: availability and purchasing in predominately rural small and large high schools. J Am Diet Assoc. 2009;109(5):857–864. Google Scholar | Crossref | Medline 49. Kimminau, KS, Murphy, KC, Huang, C. Kansas Public School Health: Nutrition, Physical Education and Physical Activity Policies and Practices. Topeka, KS: Kansas Health Institute; 2006. Google Scholar 50. Turner, LR, Chaloupka, FJ. Student access to competitive foods in elementary schools trends over time and regional differences. Arch Pediatr Adolesc Med. 2012;166(2):164–169. Google Scholar | Crossref | Medline 51. Freedman, DS, Khan, LK, Serdula, MK, Dietz, WH, Srinivasan, SR, Berenson, GS. The relation of childhood BMI to adult adiposity: the Bogalusa Heart Study. Pediatrics. 2005;115(1):22–27. Google Scholar | Crossref | Medline | ISI 52. Krebs, NF, Himes, JH, Jacobson, D, Nicklas, TA, Guilday, P, Styne, D. Assessment of child and adolescent overweight and obesity. Pediatrics. 2007;120: S193–S228. Google Scholar | Crossref | Medline | ISI 53. Demerath, EW, Schubert, CM, Maynard, LM. Do changes in body mass index percentile reflect changes in body composition in children? Data from the Fels Longitudinal Study. Pediatrics. 2006;117(3):E487–E495.
- 40. Google Scholar | Crossref | Medline | ISI 54. Himes, JH . Anthropometric indicators of obesity: epidemiologic and public health aspects of their development and use. In: Pena, M, Bacallao, J, eds. Obesity and Poverty: A New Public Health Challenge. Washington, DC: Pan American Health Organization; 2000:95–100. Google Scholar 55. Brener, ND, Wheeler, L, Wolfe, LC, Vernon-Smiley, M, Caldart-Olson, L. Health services: results from the school health policies and programs study 2006. J Sch Health. 2007;77(8):464–485. Google Scholar | Crossref | Medline | ISI 56. University of Arkansas for Medical Sciences, College of Public Health . Year two evaluation: Arkansas Act 1220 of 2003 to combat childhood obesity. Little Rock, AR: University of Arkansas: University of Arkansas for Medical Sciences; 2006. Google Scholar 57. Taras, HL, Frankowski, BL, McGrath, JW. The role of the school nurse in providing school health services. Pediatrics. 2001;108(5):1231–1232. Google Scholar | Crossref | Medline | ISI 58. U.S. Department of Health and Human Services, Health Research and Services Administration, Maternal and Child Health Bureau . Growth Charts Training: Accurate Weighing and Measuring. Rockville, MD: U.S. Department of Health and Human Services; 2006.
- 41. Google Scholar 59. Ikeda, JP, Crawford, PB. Guidelines for Collecting Heights and Weights on Children and Adolescents in the School Setting. Berkeley, CA: University of California Berkeley, Center for Weight and Health; 2005. Google Scholar 60. Gance-Cleveland, B, Bushmiaer, M. Arkansas school nurses’ role in statewide assessment of body mass index to screen for overweight children and adolescents. J Sch Nurs. 2005;21(2):64–69. Google Scholar | SAGE Journals 61. Centers for Disease Control and Prevention . The Public Health System and the 10 Essential Public Health Services . 2016. http://www.cdc.gov/nphpsp/essentialServices.html. Updated May 29, 2014. Accessed May 12, 2016. Google Scholar 62. Centers for Disease Control and Prevention . About the Division of Adolescent and School Health. 2016. http://www.cdc.gov/HealthyYouth/about/. Accessed May 12, 2016. Updated September 7, 2016. Google Scholar 63. U.S. Department of Health and Human Services, Office of Disease Prevention and Health Promotion . Healthy People 2020. 2016. https://www.healthypeople.gov/2020/topics- objectives/topic/early-and-middle-childhood/objectives. Accessed May 12, 2016. Updated September 14, 2016.
- 42. Google Scholar 64. U.S. Department of Education, U.S. Department of Health and Human Services . Healthy Students, Promising Futures: State and Local Action Steps and Practices to Improve School-Based Health. 2016. http://www2.ed.gov/admins/lead/safety/healthy- students/toolkit.pdf. Published January 2016. Accessed May 12, 2016. Google Scholar 65. Action for Healthy Kids . The Learning Connection: The Value of Improving Nutrition and Physical Activity in Our Schools. 2004. http://www.actionforhealthykids.org/storage/documents/AFHK_ The_Learning_Connection_The_Value_of_Improving_Nutrition _and_Physical_Activity_in_our_Schools_2004_- _Full_Report_011006.pdf. Accessed December 18, 2016. Google Scholar View Abstract Related Articles Citing Articles: 0 Article available in: Vol 32, Issue 3, 2018 SAGE Recommends Close Sort by What is this? Scroll to top Fetching related content... Scroll to bottom SAGE Video Streaming video collections
- 43. SAGE Knowledge The ultimate social sciences library SAGE Research Methods The ultimate methods library SAGE Stats Data on Demand CQ Library American political resources SAGE Journals About Privacy Policy Terms of Use Contact Us Help Browse Health Sciences Life Sciences Materials Science & Engineering Social Sciences & Humanities Journals A-Z Resources Authors Editors Reviewers Librarians Researchers Societies Opportunities
- 44. Advertising Reprints Content Sponsorships Permissions American Journal of Health Promotion ISSN: 0890-1171 Online ISSN: 2168-6602 Copyright © 2019 by SAGE Publications Cookies Notification This site uses cookies. By continuing to browse the site you are agreeing to our use of cookies. Find out more. Top <iframe src="https://www.googletagmanager.com/ns.html?id=GTM- 5M58KS" height="0" width="0" style="display:none;visibility:hidden"></iframe> Anywhere addJournal Add Alert s 10.1177/0890117 sage_ahpa32_70 abs Select style true
- 45. Download Citation abs RIS (ProCite, Reference Manager) Download Citation /doi/full/${article. ${article.titles.title. 9ca6ba9337334fd 1 S end Population-Level Choose Choose Choose Choose 058f11ae-cce1-45 /doi/full/10.1177/ View Large Image
- 46. Relevance S ign in S earch American College of Veterinary Pathologists [Type the document title] [Type the document subtitle] List author names [Select the date] [Abstract: Type the abstract of the HR Plan here. The abstract is typically a short summary of the contents of the document.] Table of Contents I.Executive Summary1 II.Business Strategy Report 1 III.HR Organization Design 1 V.Compensation Plan1 VI.Training and Development Plan1 VII.HR Forecast Plan2 VIII.Conclusions2 IX.Appendix2 X.References2 XI.Document Work Log2
- 47. MBA 533 – Human Resource in Management - HR Project Template Page 0 of 3I. Executive Summary You will complete this portion when the Comprehensive HR Project is submitted in Module 7. II. Business Strategy Report - 100 Points (Module 1) As a team, review and discuss the company strategy, including industry realities, competitors’ analysis, and differentiation in the market. Be sure to focus on the role of strategy in the competitive position of Motors and More. Your report should address the items below. A. Using Porter’s Five Factors Analysis of competitive position, analyze the business strategy and describe your findings. B. Review the role of strategy in company performance. What will be needed in the human resource strategy to support the company strategy? III. HR Organization Design - 100 Points (Module 2) A. Design a typical HR department and identify each HR unit. For each HR unit, provide roles/ responsibilities and job titles. Develop an organization chart of a typical HR department. B. Given the size of Motors and More, indicate which positions identified in your typical HR department should be combined or eliminated to reduce the number of HR employees. Provide new job titles and develop an organizational chart specifically for Motors and More’s new HR department. Provide the total number of staff for each HR unit. IV. Recruiting and Retention Plan - 100 Points (Module 3) A. Given the increase in product demand, how many people will you need to hire and in what functional areas (manufacturing, operations, customer service, marketing and sales, finance/ accounting, and HR)? Provide your rationale for the proposed hiring in each unit. Consider the turnover rate. Identify the factors that could be causing turnover. Identify the costs of turnover.
- 48. B. Include the types of interviews you would conduct and why. C. Develop strategies to recruit the appropriate applicants and include sources and tools used for recruiting and selection. Identify the possible areas and types of discrimination that could occur. D. What can you do to retain current employees? What are the benefits of retention? E. How will you assess the effectiveness of your recruiting efforts? V. Compensation Plan - 100 Points (Module 4) Develop a progressive yet competitive compensation plan that will support recruiting and retention efforts and lower the employee turnover rate. Traditionally, Motors and More has provided employees minimum wage and statutory benefits. A. How does Motors and More’s employee compensation compare relative to other organizations in the area? Will the organization meet, lead, or lag the local market? Explain your rationale. B. Identify alternative pay methods and discuss the advantages and disadvantages of each. C. What benefits will you offer? Include statutory benefits. What are the costs of those benefits? What is the rationale for offering those benefits? D. Develop a communications plan regarding how employees will be informed about the compensation plan. Define the sequence of communications considering the who, what, and when of the message.VI. Training and Development Plan - 100 Points (Module 5) Develop a human resource development (HRD) plan. Given the fact that Motors and More has no formal training program and promotions have been based on seniority, your plan should address: A. New-employee training. B. Current-employee training for current and future jobs according to a career path. C. Manager and supervisory training.
- 49. In your training plan, address the following: A. How will you conduct a needs assessment for each group (include methods and instruments)? B. How will training content be developed or obtained? C. How will training be delivered (e.g., classroom, intranet, blended, self-study, etc.) and by whom internal employee or external consultant/trainer)? Provide a rationale for your decision. VII. HR Forecast Plan - 100 Points (Module 6) Develop a three-year HR forecast (prediction of the future) using the following assumptions: A. Labor supply/demand will become more rigorous (demand for workers will increase, but the labor pool will remain the same or shrink). Labor costs will increase. B. Demand for Motors and More products will continue to increase. Production defects will also continue to increase. C. Motors and More’s workforce will become more diverse as the company hires more Hispanics, Kurds and persons from alternative workforces. D. The president will start another company and will hire someone to manage the daily operations of Motors and More while he takes on more of an overseeing role. E. Motors and More will decide to develop an additional product to broaden its portfolio. There is no existing capacity for the product, nor do the existing production lines meet the manufacturing requirements for the new product. VIII. Conclusions You will complete this portion when the Comprehensive HR Project is submitted in Module 7. IX. Appendix Add any supplemental information, diagrams, pictures, or forms that support your project work. X. References Include references to support your conclusions. XI. Document Work Log
- 50. Complete the table to assist in assessing the contributions made by the individual team members. Section Team Member - Primary Team Member - Secondary I. Executive Summary II. Business Strategy Report III. HR Organization Design IV. Recruiting and Retention Plan V. Compensation Plan VI. Training and Development Plan VII. HR Forecast Plan Page 2 © 2007 SHRM. Don McCain, Ed.D. 1
- 51. Society for Human Resource Management MOTORS AND MORE, INC. – A PROGRESSIVE HR CASE STUDY By Don McCain, Ed.D. Learning Objective(s) Upper-level undergraduate students will work through issues associated with developing and sustaining an HR department to support an organization facing labor shortages and high product demand. At the end of the study, students learn how to: 1. Align HR initiatives with corporate strategy. 2. Develop a complete HR organization structure, including roles and responsibilities, and then adjust the structure to support the organization. 3. Develop a basic staffing plan. 4. Develop a basic training plan. 5. Determine and support a pay and benefits plan. 6. Determine future HR requirements. CASE OVERVIEW You are hired as the HR director for the fictitious Motors and More, Inc. Motors and More, a business-to- business sales company, manufactures small motors and accessories for industrial and home products. The industry is highly competitive, and the company follows a
- 52. prospector strategy. A prospector strategy takes advantage of new markets and products (Gomez-Mejia, Galkin and Cardy, 2001). Organizational emphasis is on growth, innovation and new product development. A prospector wants to be first to market. To respond to competitive and rapidly changing markets, prospectors have flexible, flat and more decentralized organizational structures. Motors and More is headquartered in a small southern town of 28,000 people, with a low unemployment rate of 3.1 percent. This means that demand for workers exceeds the labor supply. There is a technical school and a community college within 50 miles of Motors and More. Motors and More’s president is former military and is highly patriotic. He is committed to staying in the community. Recently, several other local companies have experienced labor organizing activities. Motors and More employs 116 people. Until you were hired, there was no HR department. Recently, the organization’s employee turnover rate has been higher than normal. The marketing and sales department continues to sell products to an expanding market. Because of this increased product demand, output must be increased by 96 percent. Eighty-eight percent of Motors and More employees are Caucasian. With the exception of one female supervisor in the customer service department, the president and all other managers are Caucasian men. Management promotions have been based on seniority. The local labor market population is approximately 48 percent minority. There is a growing Hispanic
- 53. and Kurdish population that have not been accepted into the community. All the employees in manufacturing (including quality control), customer service and operations (responsible for shipping and receiving; distribution of raw materials, components parts and finished goods inventory; and maintenance and cleaning) have at least a high school degree or GED. The organization provides some skills training courses. Please refer to the organizational chart in Figure 1 for more details. © 2007 SHRM. Don McCain, Ed.D. 2 Figure 1: Motors and More Organization Chart
- 54. President HR Director Staff (TBD) Finance and Accounting 1 manager, 5 professionals and 1 hourly (includes payroll) Manufacturing 1 manager and 69 employees Quality Control 3 employees Operations 1 manager 14 employees Customer Service – inbound only 1 female supervisor
- 55. 5 CRS Marketing/ Sales 1 manager 9 salesmen Maintenance and Cleaning 1 leader 3 employees © 2007 SHRM. Don McCain, Ed.D. 3 DESIGNING THE HR DEPARTMENT A. Design a typical HR department and identify each HR unit. For each HR unit, provide roles/ responsibilities and job titles. Develop an organization chart of a typical HR department. B. Given the size of Motors and More, indicate which positions identified in your typical HR department should be combined or eliminated to reduce the number of HR employees. Provide new job titles and develop an organizational chart specifically for Motors and More’s new HR department. Provide the total number of staff for each HR unit.
- 56. Organization Design Organizing is a basic managerial function. Organizing is the process of designing jobs, grouping jobs into manageable units, and establishing patterns of authority among jobs and groups of jobs (Griffin and Moorhead, 2006). “Organization design refers to the framework of jobs, positions, groups of positions, and reporting relationships among positions that are used to construct an organization” (DeNisi and Griffin, p. 50). Organizing combines with organization design to form an organizational structure. Using Anthony, Kacmar and Perreewe (2006) as a source, Figure 2 represents a comprehensive HR structure. Some HR professionals may argue against including organization development as a part a human resource development strategy. Nonetheless, this figure is helpful because it depicts the organizational functions that must be included in a comprehensive HR department. Figure 2: An HR Organization Chart
- 57. Roles/Responsibilities and Job Titles All HR managers, regardless of their functional areas of expertise, must be able to hire, train, coach, recognize and reward performance (performance management), plan, organize, set goals, develop and implement strategies, lead employees, create and administer budgets, etc. These are responsibilities common to all managers. In addition, a decision needs to be made regarding administrative support— should it be centralized or should it be dispersed among the functional or operational areas? HR Director or Manager Roles/responsibilities goals and strategies with those of the organization. HR. HR (VP, Director, or Manager) Organization Development
- 58. Staffing or Employment Employee or Industrial Relations HRD or Training and Development Compensation Employee or Industrial Relations Health and Safety Job and Salary Administration Benefits Administration © 2007 SHRM. Don McCain, Ed.D. 4 Organization Development (OD) Possible job titles: OD specialist, OD consultant
- 59. Role/responsibilities internal contract(s). identify organizational issues with the goal of performance improvement. Issues may include the reward system or performance management, management style, structure, processes, tools and equipment, goal setting, etc. ltants to develop interventions) to address issues or problems that can be solved by collecting survey data, coaching, training; provides feedback to management and employees. achievement. Staffing or Employment Possible job titles: Employment manager, staffing manager, recruiting manager, staffing or recruiting specialist or coordinator Roles/responsibilities
- 60. Ensures they are consistent with performance management requirements. tions, résumés and references. instruments such as tests or pre- employment processes, procedures or protocols. tes. complete. . Human Resource Development (HRD) or Training and Development Possible job titles: Training specialist, training coordinator or administrator, facilitator, learning specialist, designer, developer, evaluator, training or performance consultant Roles/responsibilities HRD is responsible for the development of the organization’s
- 61. intellectual capital. HRD professionals are involved in needs assessment; design, development, delivery and evaluation of learning experiences; development of career path models; employee orientation; etc. HRD supports the performance management process by training managers and employees on performance management. Specific roles and responsibilities are discussed below. Robinson and Robinson (1996) provide some of the roles/responsibilities by job. experiences; manages group work and processes; maintains the agenda; provides feedback to learners, designers and developers. t; writes goals and objectives; defines and outlines content in conjunction with the evaluator; develops evaluation plans in conjunction with the internal client; determines instructional strategies. © 2007 SHRM. Don McCain, Ed.D. 5 oper: Develops full content and instructional strategies; develops or secures instruments, cases, assessments, etc.; develops leaders’ and
- 62. participants’ guides and materials; develops media; may conduct train-the-trainer sessions. nction with designer and client, develops and implements evaluation plans; conducts all levels of evaluation; reports evaluation findings to appropriate persons; may assess facilitator skills. ery of learning experiences; coordinates participant materials and media; enrolls participants and sends pre-course materials; secures facilities; coordinates facilities, including hotels, training rooms and breakout rooms; tracks attendance and maintains records; promotes the course or learning experiences; ships materials; tracks expenses. recipient of the services) liaison: Conducts organizational analyses for internal client organization; contracts for performance improvement; consults with internal clients on performance issues; prioritizes needs; secures support (including funding; access to subject matter experts; collects audience profiles; supports learners’ participation; supports transfer of new knowledge and skills to the job; has access to data necessary to carry out these responsibilities); with client input, selects facilitators; provides feedback to internal clients; manages the interface with the HRD staff.
- 63. Compensation has two primary areas—benefits and salary administration. In many organizations, payroll is a function of the accounting department. In other organizations, payroll is placed in compensation. Benefits Job titles: Benefits analyst, benefits specialist, benefits administrator Roles/responsibilities to the internal requirements of staff versus the competition and to retain employees. Administers the health plan (including HMO or PPO plans). contribution or defined benefit plans. Salary Administration Job titles: Job analyst, job and salary analyst or specialist Roles/responsibilities merit, incentives, bonuses, gain sharing, profit sharing, stock options and other rewards.
- 64. competition with the goal to lead, lag or meet the competition. responsibilities, job specifications and pay grades. goals and standards; supports the performance management process. adjustments to pay grades based on survey results. © 2007 SHRM. Don McCain, Ed.D. 6 Employee Relations or Industrial Relations Job title: Employee relations specialist Roles/responsibilities
- 65. relations issues. es employee survey results. Develops and implements plans to address identified issues. -free environment. cipline procedures. issues (EAP role). maintains “ethics” hotline. n with staffing, supports relocation and outplacement services. employees. Health and Safety Job titles: Safety specialist, safety coordinator, safety
- 66. administrator, industrial nurse Roles/responsibilities environment. aining. OSHA requirements. on the job. provided for the facility. Prospector Strategy A strategy is a plan for interacting with the competitive environment to achieve organizational goals (Daft, 2003). According to Gomez-Mejia, Balkin and Cardy (2004), the objective of a prospector strategy is to find and exploit new products and market opportunities. Organizations that use a prospector strategy are aggressive in the marketplace, highly competitive and quick to produce new products and services to be the first to market. Their key objective is to find and exploit new products and market opportunities. They operate in an environment of uncertainty and instability.
- 67. Organizational practices inherent in a prospector strategy include (Gomez-Mejia, Balkin and Cardy, 2004): on faster innovation, flexibility and creativity. making the decision. development purposes. -based and cross-functional training. To be flexible, organizational structures in a prospector strategy are flat in organization design, decentralized and/or team-based. © 2007 SHRM. Don McCain, Ed.D. 7 DEVELOPING THE RECRUITMENT AND RETENTION PLAN
- 68. A. Given the increase in product demand, how many people will you need to hire and in what functional areas (manufacturing, operations, customer service, marketing and sales, finance/ accounting, and HR)? Provide your rationale for the proposed hiring in each unit. Consider the turnover rate. Identify the factors that could be causing turnover. Identify the costs of turnover. B. Include the types of interviews you would conduct and why. C. Develop strategies to recruit the appropriate applicants and include sources and tools used for recruiting and selection. Identify the possible areas and types of discrimination that could occur. D. What can you do to retain current employees? What are the benefits of retention? E. How will you assess the effectiveness of your recruiting efforts? The Selection Process This is a good time to review the selection process. According to Noe, Hollenbeck, Gerhart and Wright (2007), the steps in a selection process include screening applications and résumés; reviewing and testing work samples; interviewing candidates; checking references and background; and making a selection. Internal candidates would not require all of these steps. Turnover The Department of Labor uses the following formula to measure turnover:
- 69. ( Number of separations during the month Total number of employees at midmonth ) x 100 Separations = those leaving the organization Motors and More is not experiencing involuntary turnover, however. The organization is expanding its workforce, and the community is experiencing a labor shortage. The turnover, then, is voluntary. Some reasons for voluntary turnover include: —work overload, issues with the manager or other employees, little flexibility in work scheduling, lack of challenge. —employees can easily find alternative employment because of the high demand for employees in the area. —competitive pay and benefits, no career path, perceived unfairness in rewards distribution. nal or family reasons.
- 70. Turnover is expensive for organizations: Employee Separation Costs Recruiting Costs Selection/ Interviewing Costs Training Costs Less Direct Costs • Severance pay • Benefits • Unemployment insurance costs • Exit interview • Outplacement • Legal fees • Advertising • Recruiter’s and manager’s time • Travel (applicant and/or recruiter) • Search firm • Employee referral fees
- 71. • Campus visits • Interviewing: cost of employees’ time • Cost of travel: cost of travel for applicant to the interview • Instrument development (questions, • Training new employee (orientation, job, team) • Travel for training • Trainer’s time • Lost productivity during training • Training materials • Lost productivity due to new employee’s productivity curve or the existing staff taking on more work while being less efficient/ effective while the
- 72. © 2007 SHRM. Don McCain, Ed.D. 8 criteria, tests) • Reference checks • Background checks • Relocation • Pre-employment medical • expenses • Coaching time vacancy exists. • Overtime for current employees • Loss of business due to poor customer service • Not being able to take on new business due to lack of resources • Lost knowledge
- 73. Equal Pay There is one supervisor who is a woman and four managers, all of whom are men. Motors and More should examine the jobs to determine if they are equal in terms of skill (experience or training), effort (mental or physical effort), responsibility (degree of accountability) and similar working conditions (physical surroundings or hazards). Is there enough difference between the positions to warrant a “supervisor” job classification and not “manager” job classification? If job responsibilities (such as outbound sales) expand, will the job classification difference still be warranted? Sex Discrimination Why is there only woman in a lower management position supervising the call center? It may appear that Motors and More believes there are certain jobs better suited for women. Was gender a factor in the hiring decision? Is stereotyping occurring? Racial/Ethnic Discrimination Motors and More is 88 percent Caucasian, and all managers are men. The local population is 48 percent minority, indicating possible discrimination. Since promotions are based on seniority, it appears that Caucasian men have been there the longest and received the promotions. Motors and More must aggressively recruit, staff and promote qualified minorities. It should also promote based on performance and job specifications, not tenure. Because of Motors and More’s racial demographics, we can assume that the local Hispanic and Kurd
- 74. population has not been accepted at Motors and More. This lack of inclusion may lead to discrimination allegations. Benefits of Retention Organizations with good retention: s, which can provide a competitive advantage. become available, thereby reducing recruiting and training costs. because employees know their jobs, peers, products and customers. performance. goals. Can become an employer of choice, reducing recruiting and turnover costs. Assessing the effectiveness of recruiting efforts There are a number of ways to assess effectiveness of recruiting efforts. One way is to calculate costs per hire. To calculate costs per hire, add total recruiting costs and divide by the number of candidates hired.
- 75. © 2007 SHRM. Don McCain, Ed.D. 9 A second method is to determine the yield ratio. According to Mathis and Jackson (2006), the yield ratio is the comparison of the number of candidates at one stage in the recruiting process to the number of candidates at another stage. To calculate a job offer yield ratio, divide the number of applicants by the number of applicants offered a job. You can also use a selection rate to assess your recruiting efforts. A selection rate is the percentage hired from a given group of candidates. It equals the number of employees hired divided by the number of applicants (Mathis and Jackson, 2006). Mathis and Jackson (2006) also discuss acceptance rate (the percentage of job offers rejected) and success rate (comparing the number of past candidates who were good performers to current employees). You can also identify effective recruiting sources by determining where you found candidates who can be defined as good employees. You may also try to determine which recruiting sources provide higher-quality applicants. For example, many organizations regularly recruit from certain universities because, over time, those universities have provided the organization with higher-quality candidates than other schools.
- 76. © 2007 SHRM. Don McCain, Ed.D. 10 DEVELOPING A COMPENSATION PLAN Develop a progressive yet competitive compensation plan that will support recruiting and retention efforts and lower the employee turnover rate. Traditionally, Motors and More has provided employees minimum wage and statutory benefits. A. How does Motors and More’s employee compensation compare relative to other organizations in the area? Will the organization meet, lead or lag the local market? Explain your rationale. B. Identify alternative pay methods and discuss the advantages/disadvantages of each. C. What benefits will you offer? Include statutory benefits. What are the costs of those benefits? What is the rationale for offering those benefits? D. Develop a communications plan regarding how employees will be informed about the compensation plan. Define the sequence of communications considering the who, what, and when of the message.
- 77. Merit Pay Merit pay rewards employees for work already done, usually over the last performance year. Employees are familiar with merit pay, and there is little resistance offering it. Over time, merit pay increases employees’ base pay, thereby increasing organizational costs. It is also difficult to really link performance to merit pay. Further, merit pay may not result in increased performance. Employees may not see the link between merit pay and their performance. Incentives and Bonuses Incentives and bonuses reward individual performance without adding to base salary. Incentives and bonuses also link pay with performance. For example, in manufacturing, a straight piecework plan pays employees a certain amount for each unit produced. In a team environment, a group incentive could increase group productivity. A disadvantage is that it may cause unhealthy competition among employees. Commissions Typically, commissions are pay based on product sales. On a straight commission pay plan, pay is based on employee performance; the more sales, the more commission the employee receives. A combined commission pay plan pays a base salary plus commission. Commission pay plans directly link pay to performance. Commissions can result in increased sales. Commission pay plans, however, may cause employees to behave unethically in order to make the sale. Generally, commissions reward individual, not team performance.
- 78. On-the-Spot Awards On-the-spot awards instantly reward employees for good performance or behavior. The recipient is usually nominated by a supervisor or peers. Awards may include gifts, gift certificates or cash. On-the- spot awards focus employee attention on organizational goals and objectives. In addition, employees can quickly see the link between performance or behavior and the reward. On-the-spot awards can lead to feelings of resentment or unfairness, however, if managers use their own criteria for giving awards. Gainsharing In a gainsharing incentive compensation plan, employees are rewarded for cost reduction or improved productivity. Savings are usually shared equally between the employees and the company. Organizations using gainsharing incentives usually have participative management styles. Gainsharing plans can help employees understand what is important to the organization, such as decreasing labor costs. Gainsharing can also increase employee cooperation because employees are rewarded equally, reducing competition. Gainsharing also reinforces continuous improvement. Gainsharing, however, can make it difficult to determine a productivity baseline. It can also be difficult to determine who will participate in the program. In a gainsharing plan, an organization could pay for cost reductions even when profits are declining. Lastly, since all employees are rewarded equally, the payment may not seem fair to all employees.
- 79. © 2007 SHRM. Don McCain, Ed.D. 11 Profit Sharing In profit sharing, the organization pays employees above and beyond their base pay when the organization earns a profit. Profit sharing allows the organization to reward employees when the organization can most afford it. Profit sharing also provides flexibility in the distribution of the payments. Employees may not see the link between individual performance and profits, however, minimizing the link to performance. These pay methods add value to the company while providing flexibility in pay. When suggesting possible solutions, students may offer, as an option, issuing stock. However, the instructor should advise students that Motors and More is not a public company. Deciding What Benefits to Offer Currently, Motors and More employees receive only statutory employment benefits. Statutory benefits are Social Security, workers’ compensation, unemployment compensation and FMLA leave. Social Security provides retirement and disability income and can supplement unemployment insurance. It is funded by equal contributions between the employer and the employee. Workers’ compensation covers medical costs and employee pay if the employee is unable to work due to
- 80. a job-related illness, injury or disability. It is paid for by the organization. Unemployment compensation provides income to employees who lose their jobs. The employer pays for unemployment compensation based on the organization’s location and history of terminations and layoffs. The Family Medical Leave Act requires employers with 50 or more employees to allow employees to take up to 12 weeks of unpaid leave during a 12-month period for narrowly defined personal and family health issues. The Act ensures that the employee can return to the same position or one of equal status and pay. In addition, the Act requires employers to maintain employee’s health coverage (if offered). 17 Communication plan Developing a communication plan ensures that everyone understands benefits offerings. Figure 3 provides a sample communication plan structure targeting only the employee level. Figure 3: Communication Plan Audience Message Medium Desired Result Timing Frequency Person Responsible Employees Explanation of benefits Large group meeting
- 81. Employees will understand the new benefits so they can make an informed decision Employee enrollment At enrollment time Quarterly HR Director Benefits Consultant Website Understanding the new benefits Continuous Continuous Webmaster Benefits Consultant Understanding the new benefits Based on publication dates Semi- annual Editor
- 82. Benefits Consultant One-on-one consultation Employees will understand the new benefits so they can make an informed decision Employee enrollment By appointment Ongoing Benefits Consultant © 1998 Performance Advantage Group © 2007 SHRM. Don McCain, Ed.D. 12 Different communication mediums (or methods) should be used for different audiences. The management team may require group and/or one-on-one meetings. Employees will want to see the details in a document they can read and revisit. Desired results are also audience-specific. For example, you
- 83. will want management to understand the new benefits, enroll in the plans and also be supportive of the plans. You will want employees to understand the new plans, with enrollment as the desired result. A communication plan considers timing (when the message will be communicated) and frequency (how often the message or a version of the message will be presented to the audience). For example, for benefits enrollment, timing may be one month before the enrollment period begins. The frequency may be once a week to start, increasing to twice a week as the enrollment period draws to a close. For a communication plan to succeed, each person assigned to execute each phase of the plan must be held responsible to complete it within the time specified. © 2007 SHRM. Don McCain, Ed.D. 13 DEVELOPING A HUMAN RESOURCE DEVELOPMENT PLAN Develop a human resource development (HRD) plan. Given the fact that Motors and More has no formal training program and promotions have been based on seniority, your plan should address: A. New-employee training.
- 84. B. Current-employee training for current and future jobs according to a career path. C. Manager and supervisory training. In your training plan, address the following: A. How will you conduct a needs assessment for each group (include methods and instruments)? B. How will training content be developed or obtained? C. How will training be delivered (e.g., classroom, intranet, blended, self-study, etc.) and by whom internal employee or external consultant/trainer)? Provide a rationale for your decision. New-employee Training New employees should undergo an orientation program. Comprehensive orientation should include information about the industry, organization, job unit and position. To retain employees, orientation to the team (job unit) and position are important. New-employee orientation should address individual employee goals. New employees may also need specific job training to enhance their skills, to safely use equipment and to follow procedures. Current-employee Training Current employees may need refresher skills training and diversity training. Evaluate whether English-as- a-second language (ESL) training would support the work environment. If functional career paths are developed, training should align to the functional career path. Because Motors and More will likely add to team leaders, basic supervisory and team leadership training may be needed.
- 85. Manager and supervisory Training Managers and supervisors were promoted by seniority, and there is no indication they have had any management level training. Promotion by seniority also resulted in a lack of women and minorities in top- level positions. Basic management training in areas such as budgeting and forecasting, employment laws, performance management, goal setting, and giving and receiving feedback would improve their capabilities. Diversity training is also recommended for this group. Needs Assessments Needs assessments should be conducted at the organizational, job and individual levels. At the organizational level, a needs assessment should assess current and future training needs, identify existing gaps and recommend specific training and development required to close the gaps. An organizational needs assessment is client-based and considers organizational objectives and strategies. A job (or task) needs analysis identifies the specific skills, knowledge and abilities (KSAs) needed to perform the tasks in a current or future position (Jackson and Schuler, 2006). A job analysis identifies the training requirements for the job. Additional sources include interviewing the incumbent and the incumbent’s manager to identify specific skills, knowledge and behavior required to successfully do the job. The goal of a job needs analysis is to define what successful performance looks like and identify the KSAs required. An individual needs assessment identifies the KSA gaps
- 86. between existing and required performance. A good method to assess individual needs is to measure performance against objectives. This is discussed in the performance review where strengths and weaknesses can also be identified. Observation is another way to conduct this needs assessment. Needs assessments can be conducted by examining the existing (or extant) data, conducting individual interviews or focus groups, implementing surveys, using multi- rater assessments, assessing employees through various tests, and reviewing individual, functional unit and organizational performance records. © 2007 SHRM. Don McCain, Ed.D. 14 How will training content be developed or obtained? Training content can be developed or purchased. Some training may need to be developed internally. If so, given the limited HR staff, how will this be done? Using SMEs and/or an outside trainer is a possibility. Buying training programs off-the-shelf is also an option. However, off-the-shelf training products are generally not customized to the individual organization. Consequently, customization costs must be considered. Cost, time to delivery and size of target audience are also factors to consider. How will training be delivered (e.g., classroom, intranet,
- 87. blended, self-study, etc.) and by whom (internal employee or external consultant/trainer)? It is important to match delivery methods to content and audience. Some training (such as new employee orientation) can be self-study; employees can receive individual training material as such as workbooks or CDs. Some of the new-employee orientation, though, may need to be classroom-based. If the target audience has computer access, training can be delivered by Intranet, internet or CD. Classroom training is always an option, but timing and space may be issues. When planning training, keep in mind that managers and professionals usually have more flexibility in their schedules than hourly employees do. This will affect classroom delivery. Consider using job assignments and job rotation to provide depth and breadth of training. Some criteria or decision factors in training delivery include: designers and facilitators. —it takes longer to develop an online course than a classroom exercise. organization needs to be trained in remote
- 88. locations and quickly, you may need outside resources. What processes and instruments will you use to evaluate the program’s effectiveness for each group? Kirkpatrick’s four levels of evaluation is the model generally used for training evaluation. These levels are discussed extensively in Evaluating Training Programs: The Four Levels and are summarized here for your reference. Level 1: Reaction Level 1 assesses participants’ reaction to the training. Participants are asked to complete a survey at the end of the training. The survey asks participants to indicate if training objectives were met, rate facilitator skills, assess the relevancy of content and rate the appropriateness of instructional/learning strategies, materials, group interaction, etc. Level 2: Measure learning Was there a change in knowledge, skills or attitudes? Learning can be measured through tests for knowledge, assessments of performance during role-plays, demonstrations, case studies, projects, work products, etc. These instruments, developed specifically for the training, are used during the learning and feedback is provided during the learning activities. To accurately assess a shift in learning, there a baseline must be established by administering a pre-test and post-test. Level 3: Assess behavior change on the job
- 89. This is also referred to as transfer. Are participants using the new knowledge and skills on the job? To what extent? To assess this, HRD professionals can follow up on performance contracts, action plans, work products and similar transfer strategies to determine the extent to which these are being completed. HRD professionals can also conduct individual interviews of training participants, their managers and/or peers or conduct focus groups to determine transfer. Surveys can also be used. © 2007 SHRM. Don McCain, Ed.D. 15 Another consideration in assessing learning transfer involves the environment. To what extent does the environment enable or hinder the use of the new KSA? The same assessment methods can be used. Level 4: Measure results Measure any changes in the initial business metric addressed by the training. Did the metric (sales, defects, turnover, etc.) change? The return on investment (ROI) can be calculated if the dollar value of the change in the metric (benefit) and total program costs are known. When measuring results, it is important that only results due to training are considered. To do this,