(1) A single complete denture occludes against some or all of the natural teeth in either jaw. It is more common for the maxillary denture to oppose natural mandibular anterior teeth.
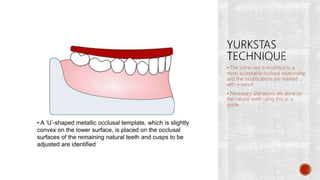
(2) Evaluation of the dentulous arch involves assessing the number, position, and condition of remaining teeth. The occlusal plane may need correction by modifying teeth.
(3) Swenson's technique uses a template made from an altered stone cast to guide reduction of teeth, correcting the occlusal plane before impressions and jaw relations are recorded.





























































![SINGLE COMPLETE DENTURES sam [Autosaved] (1).pptx](https://cdn.slidesharecdn.com/ss_thumbnails/singlecompletedenturessamautosaved1-250109094738-6d16d65c-thumbnail.jpg?width=640&height=640&fit=bounds)


































