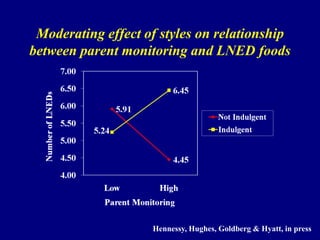
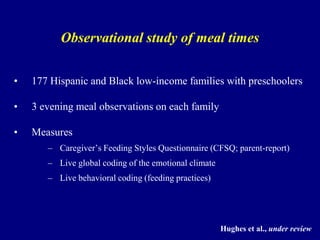
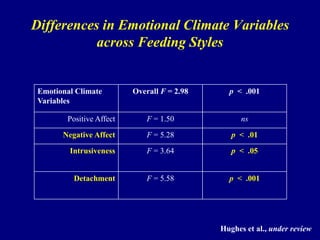
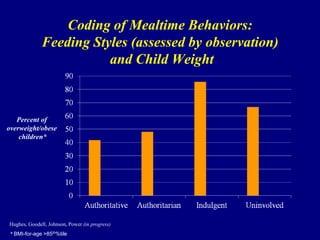
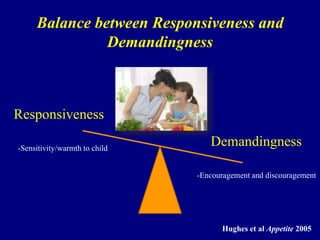
Download to read offline
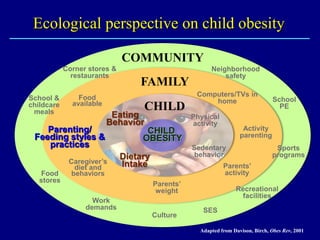

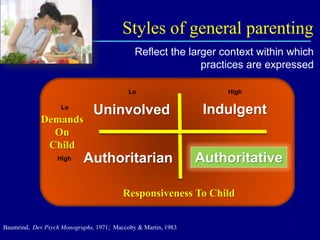
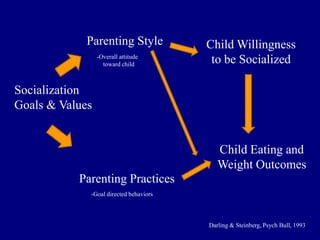
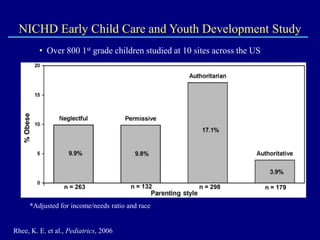
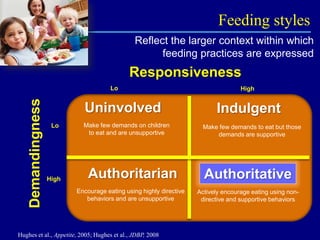
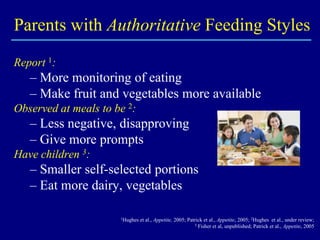
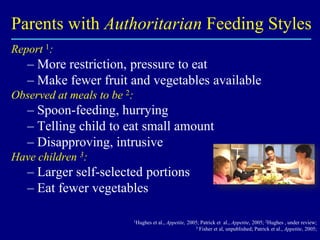

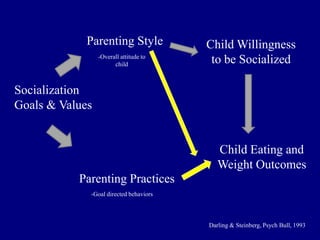
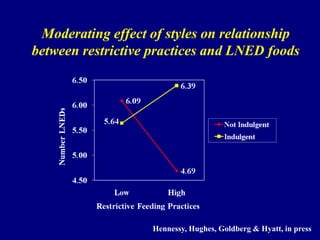


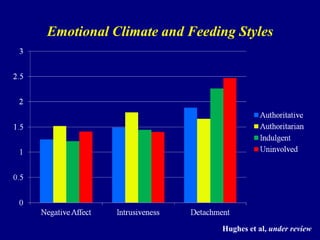
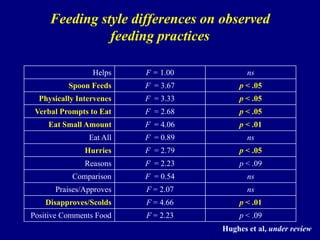
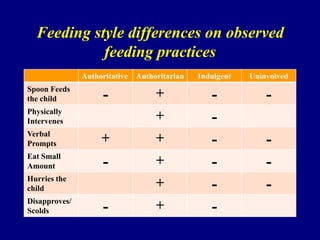



This document discusses research on how parenting styles and feeding styles influence children's eating behaviors and risk of obesity. It finds that an authoritarian parenting style and an indulgent feeding style are associated with less optimal child eating and higher risk of obesity. The research is based on studies of low-income minority families. Observational research confirms that indulgent parents are more detached during meals, while authoritarian parents show more negative behaviors like scolding. This research aims to better understand family dynamics during mealtimes that influence children's eating habits and weight outcomes.



















































































