Download as PDF, PPTX

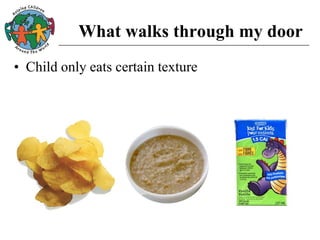
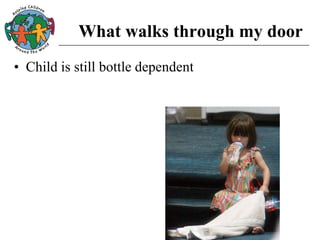
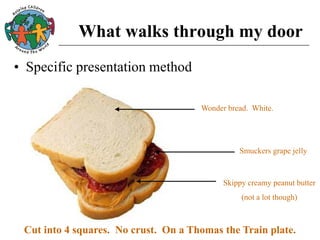

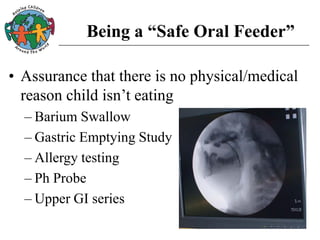


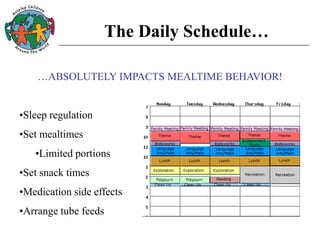
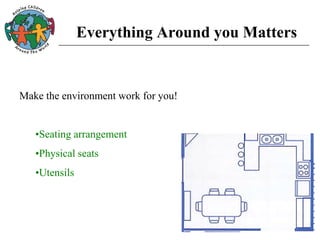
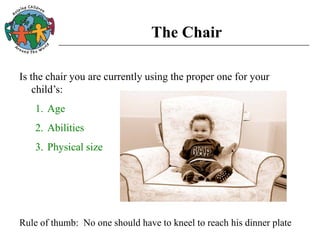

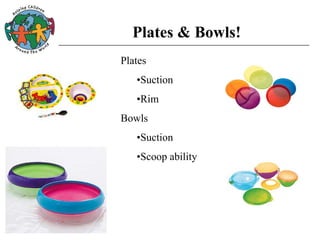
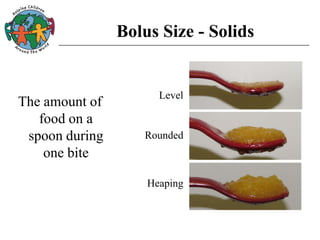
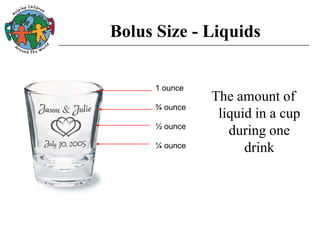
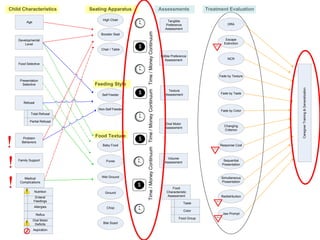


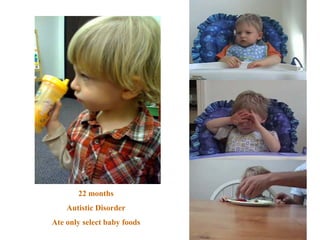

This document discusses strategies for introducing new foods to children with feeding disorders or developmental disabilities. It begins by explaining the importance of assessing a child's preferences, medical factors, oral motor skills, and problem behaviors before beginning interventions. Behavioral techniques like using highly preferred rewards, adjusting bolus size and texture, and creating an optimal eating environment can help motivate children to try new foods. The goal is to introduce foods gradually based on assessments while addressing any underlying medical or behavioral issues influencing feeding.





![Presentation 1 ellen_rome[1]](https://cdn.slidesharecdn.com/ss_thumbnails/presentation1ellenrome1-160412185420-thumbnail.jpg?width=640&height=640&fit=bounds)



























































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)




