Downloaded 767 times























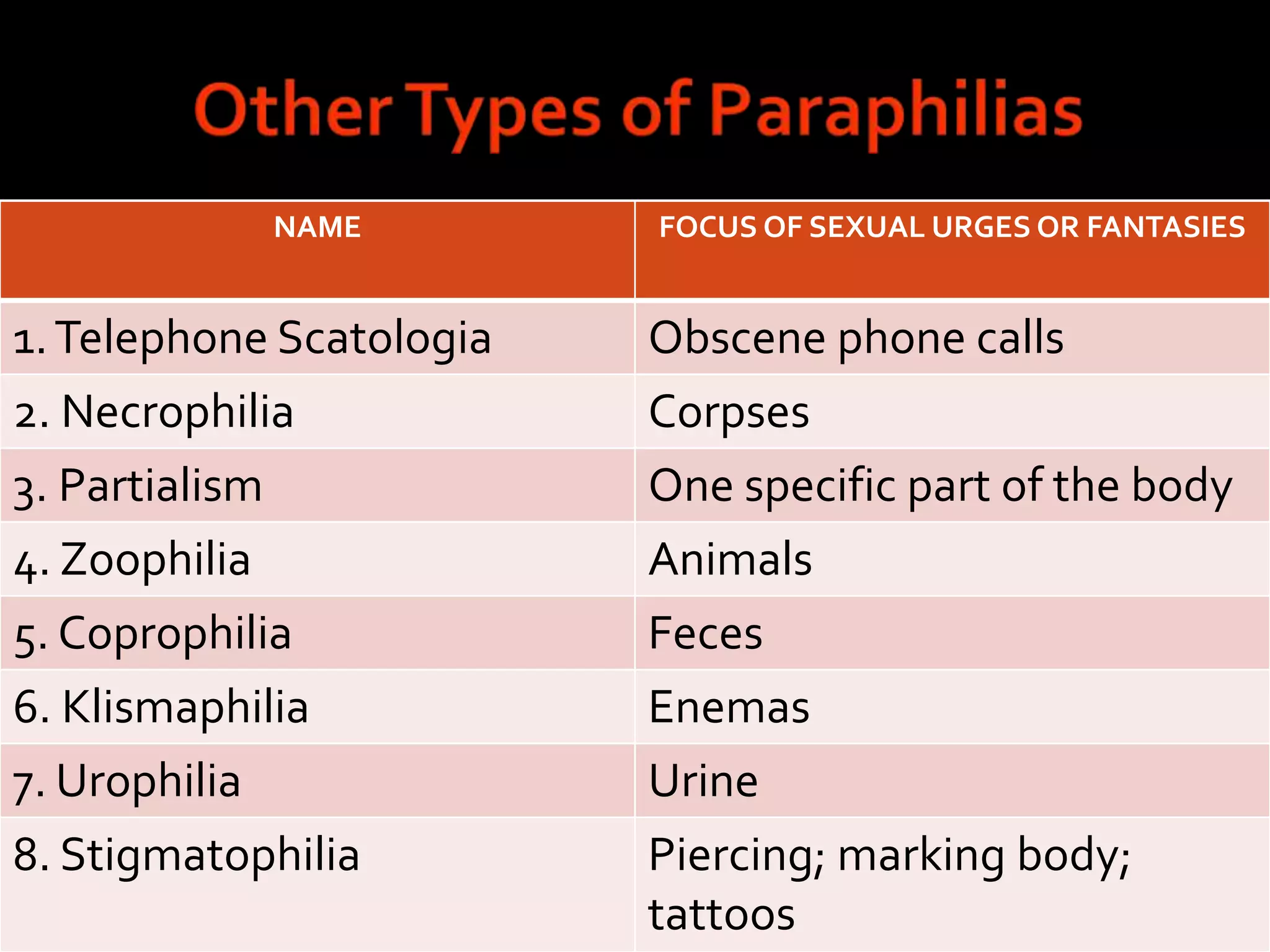






































Loving relationships contribute greatly to happiness, and sexuality influences who we fall in love with and mate with. The document discusses three categories of sexual disorders - paraphilias, gender dysphoria, and sexual dysfunctions. Paraphilias involve recurrent sexual fantasies or behaviors involving nonconsenting persons or harm. Gender dysphoria involves discomfort with one's sex. Sexual dysfunctions involve impaired sexual desire, arousal, orgasm or pain. Causes may be biological or psychological and treatments involve counseling, medication or therapy.















![Somatic Symptom and Related Disorders [2020]](https://cdn.slidesharecdn.com/ss_thumbnails/ssrdv1-200526002841-thumbnail.jpg?width=640&height=640&fit=bounds)







































![Sexual disorder [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/sexualdisorderautosaved-180531133700-thumbnail.jpg?width=640&height=640&fit=bounds)