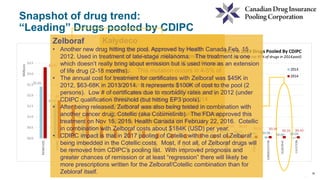
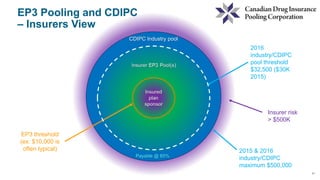
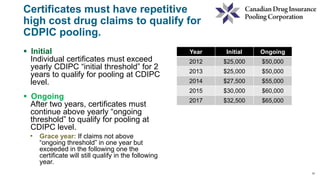
CDIPC manages high drug costs for the insurance industry through two pooling levels. The EP3 pool covers individual plans for claims above a threshold, usually $10,000. The CDIPC industry pool then covers recurring claims over $32,500 across the insurance industry. This system allows for affordability, availability, and transferability of drug coverage. In its fourth year, CDIPC has pooled over $24 million in claims and helped insurers manage unpredictable drug costs. However, new specialty drugs like Kalydeco continue driving costs higher, presenting ongoing challenges for CDIPC.



![13
13
Insurance Company “A” has an EP3 plan which pools claims at the individual
level / certificate level at $10,000 (somewhat typical)
Example of an eligible certificate hitting EP3 then CDIPC industry pool (in 2nd
year of exceeding CDIPC initial threshold of $65,000):
Family Member Paid Claims
Amount
A) “Direct” plan
sponsor claims
experience
B) Amount flowing to
insurer’s EP3 pool
[ with CDIPC ongoing threshold
@ $32.5K ]
C) Amount flowing to
CDIPC industry pool
Certificate Holder $300 $300 $0 $0
Spouse $102,000 $9,700 $22,500 $69,800
Child $50 $0 $0 $50
Allocations $102,350 $10,000 $22,500 $72,350 @ 85% =
$61,498
Example](https://image.slidesharecdn.com/session7-cdipcoverviewdanberty-160427132449/85/Session-7-13-320.jpg)