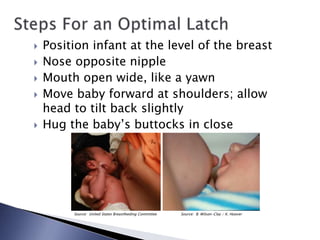
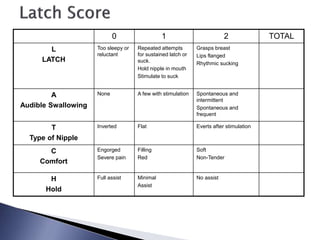
This document provides information on helping with breastfeeding, including demonstrating breastfeeding positions, signs of an effective latch, and signs of milk transfer. It discusses the benefits of skin-to-skin contact and immediate breastfeeding after birth. Signs that assistance may be needed include a LATCH score less than 7 or nipple trauma/pain. Healthcare providers should support effective positioning and latching to promote breastfeeding success and maternal comfort.