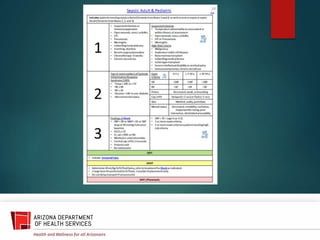
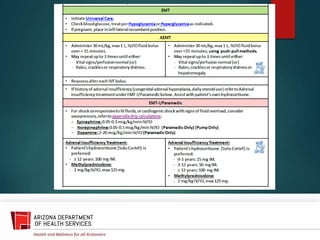
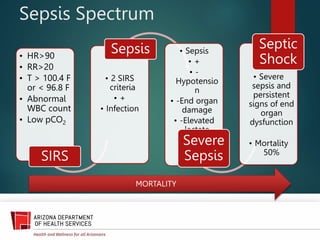
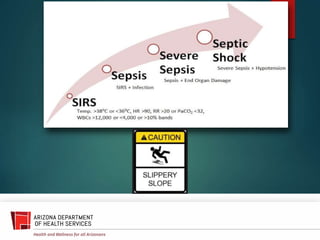
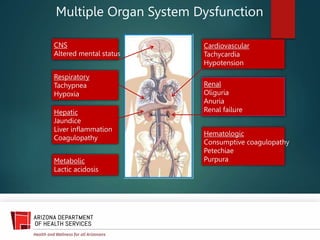
This document discusses identification and management of sepsis in the prehospital environment. It defines sepsis as an exaggerated immune response to infection that can lead to organ dysfunction. Early signs may be nonspecific but include fever, altered mental status, and fast heart rate and breathing. Prehospital treatment involves giving fluids and communicating the suspicion of sepsis to the receiving hospital. Maintaining oxygen levels and treating shock are priorities as sepsis can progress rapidly to organ failure. Monitoring end-tidal carbon dioxide and checking for lactacidosis provide valuable information.

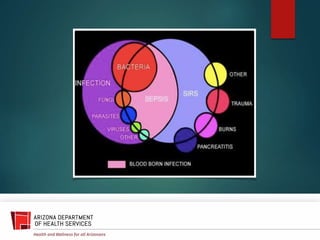



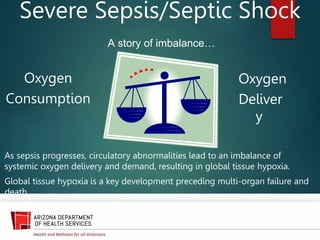
![(Crit Care Med 2006;34[6]:1589.)](https://image.slidesharecdn.com/sepsis-230829104410-d1860a3d/85/sepsis-pptx-20-320.jpg)