Downloaded 44 times

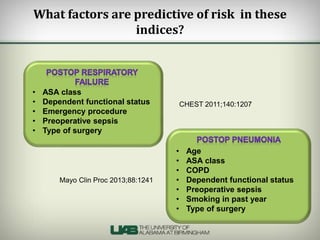
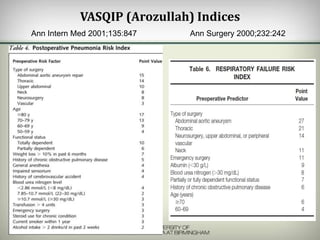
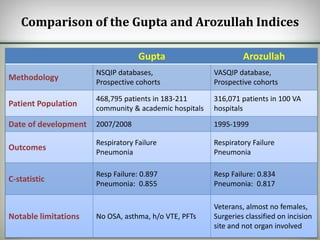

The document discusses the predictive tools for postoperative pneumonia and respiratory failure, specifically the National Surgery Quality Improvement Program (NSQIP) risk calculator known as the Gupta criteria and the Vascular Surgical Quality Improvement Program (VASQIP) indices. It compares their predictive performance and highlights that the Gupta indices offer better specificity and contemporary relevance. Notable limitations of both tools include exclusion of certain conditions and diverse patient populations.























































































