Downloaded 10 times

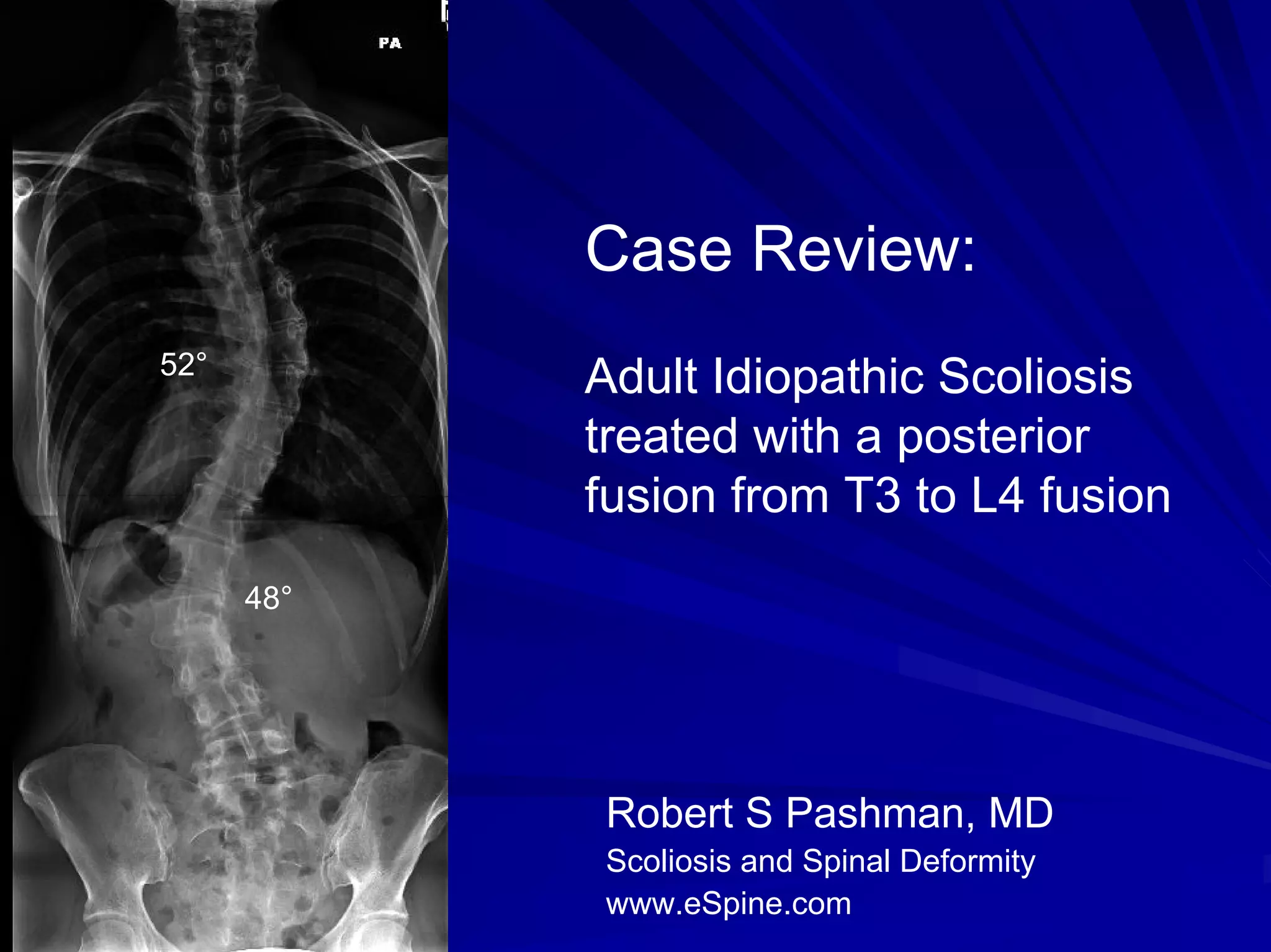
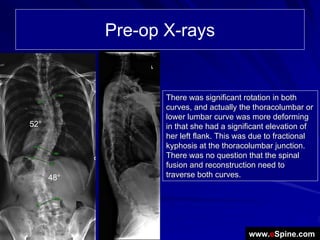
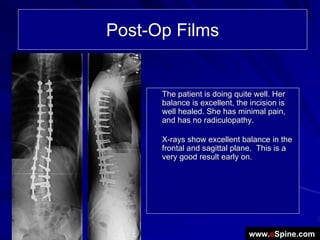
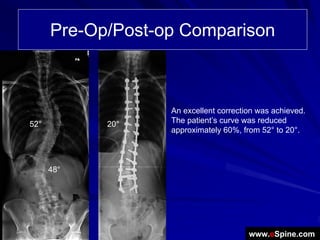
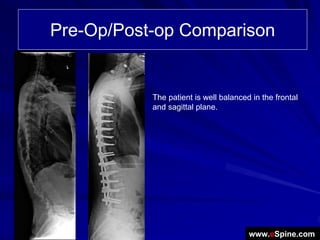

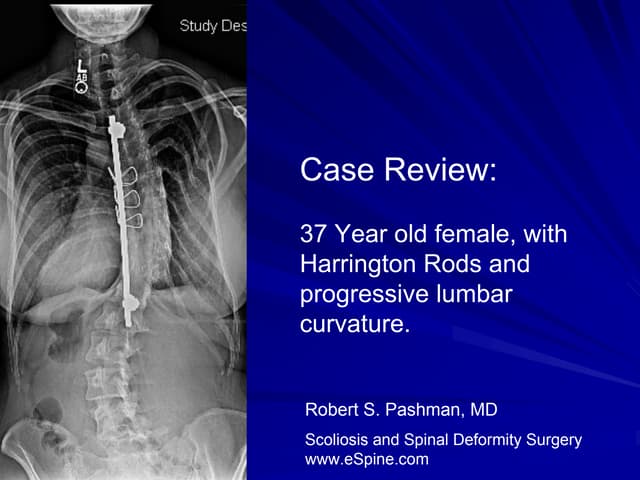
The document reviews a case of a 38-year-old female with adult idiopathic scoliosis who underwent a posterior spinal fusion from T3 to L4 after conservative treatments failed. The surgery involved significant instrumentation and osteotomies, resulting in a successful reduction of her curvature from 52° to 20°, with excellent post-operative balance and minimal pain. Pre- and post-operative x-rays indicate significant improvement in her spinal alignment and overall condition.



















































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)






![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)




