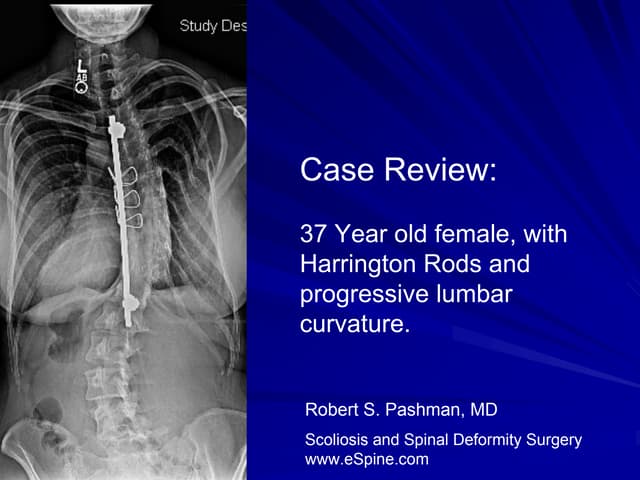
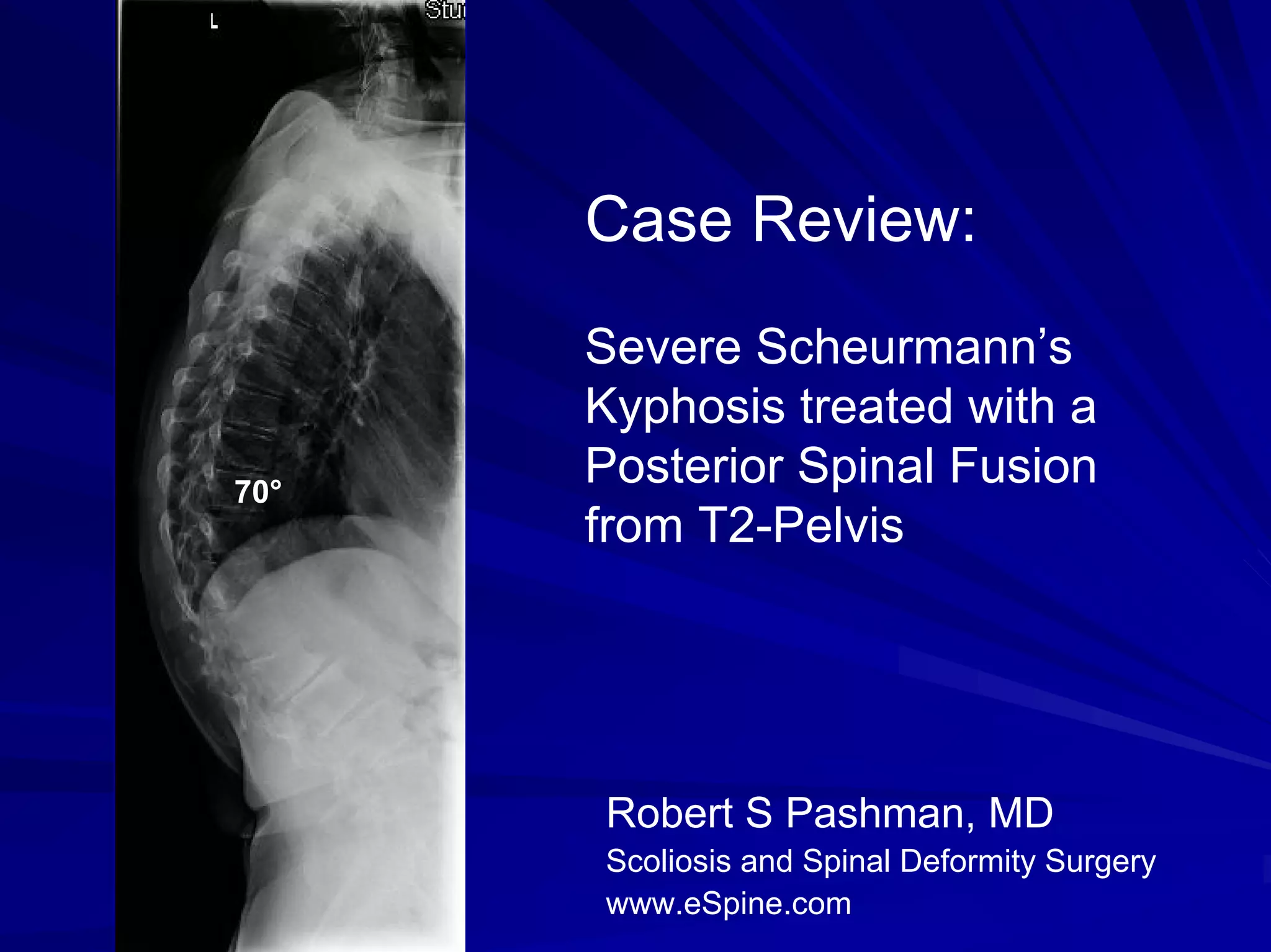
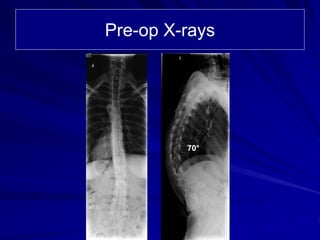
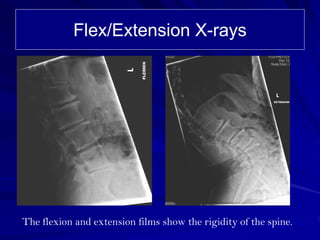
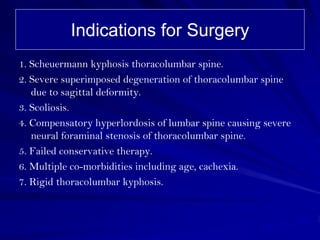
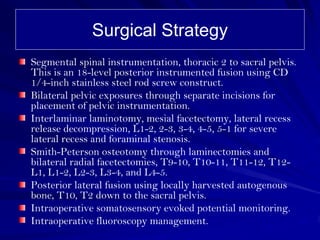
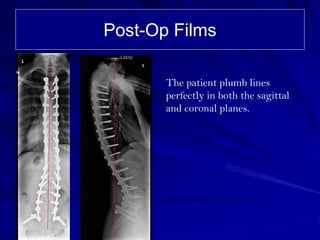
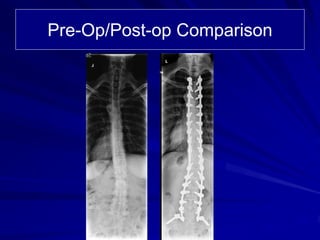
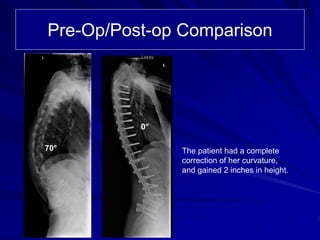

A 58-year-old female with severe rigid thoracolumbar kyphosis due to Scheuermann's disease and degeneration underwent a posterior spinal fusion from T2 to the pelvis. She had a 70 degree curvature that was rigid. The surgery involved segmental spinal instrumentation, multiple osteotomies to correct the curvature, decompression of neural elements, and an 18-level posterior fusion. Post-operatively, the patient's curvature was fully corrected and she gained 2 inches in height.