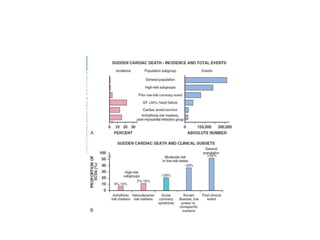
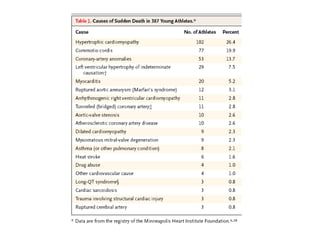
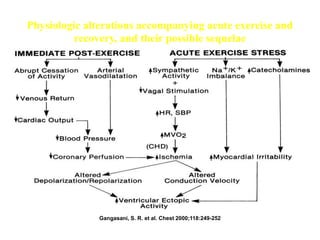
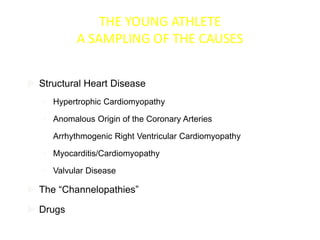
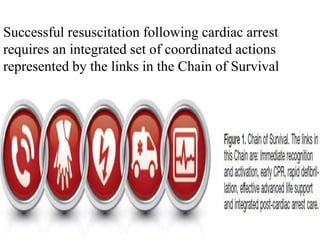
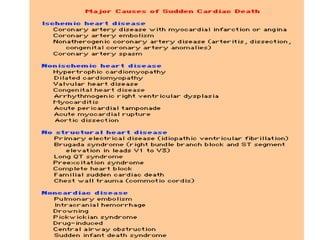
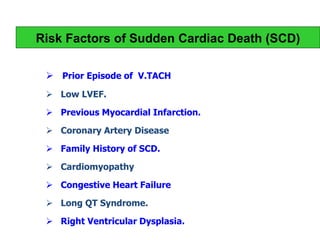
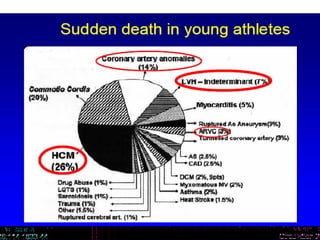
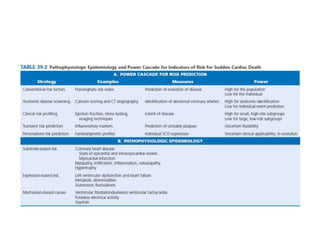
The document discusses sudden cardiac death (SCD) in various populations. It notes that SCD accounts for 12-15% of natural deaths and almost 90% have cardiac causes. The peak ages for SCD are within the first year of life and between 45-75 years. The most common causes of SCD in children are congenital heart defects while in those over 35 it is coronary heart disease. Rare causes like hypertrophic cardiomyopathy also contribute to SCD in young adults. Exercise-related SCD is often due to congenital anomalies or premature heart disease in young and older athletes respectively.





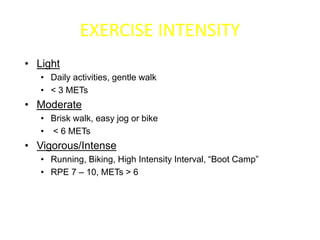

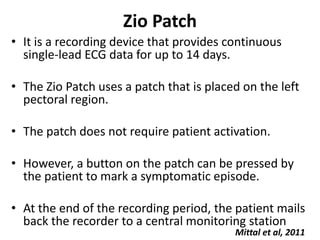




![• The incidence of sudden death has two
• peak ages: within the first year of life
(including
• sudden infant death syndrome [SIDS]; see
• Chapter 62) and between 45 and 75 years of
• age. Among the general populations of infants
• younger than 1 year and middle-aged or older
• adults, the incidence is surprisingly similar](https://image.slidesharecdn.com/scdautosaved-160131121816/85/Scd-71-320.jpg)
![• The incidence of sudden death has two
• peak ages: within the first year of life
(including
• sudden infant death syndrome [SIDS]; see
• Chapter 62) and between 45 and 75 years of
• age. Among the general populations of infants
• younger than 1 year and middle-aged or older
• adults, the incidence is surprisingly similar](https://image.slidesharecdn.com/scdautosaved-160131121816/85/Scd-72-320.jpg)

































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)







![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)





