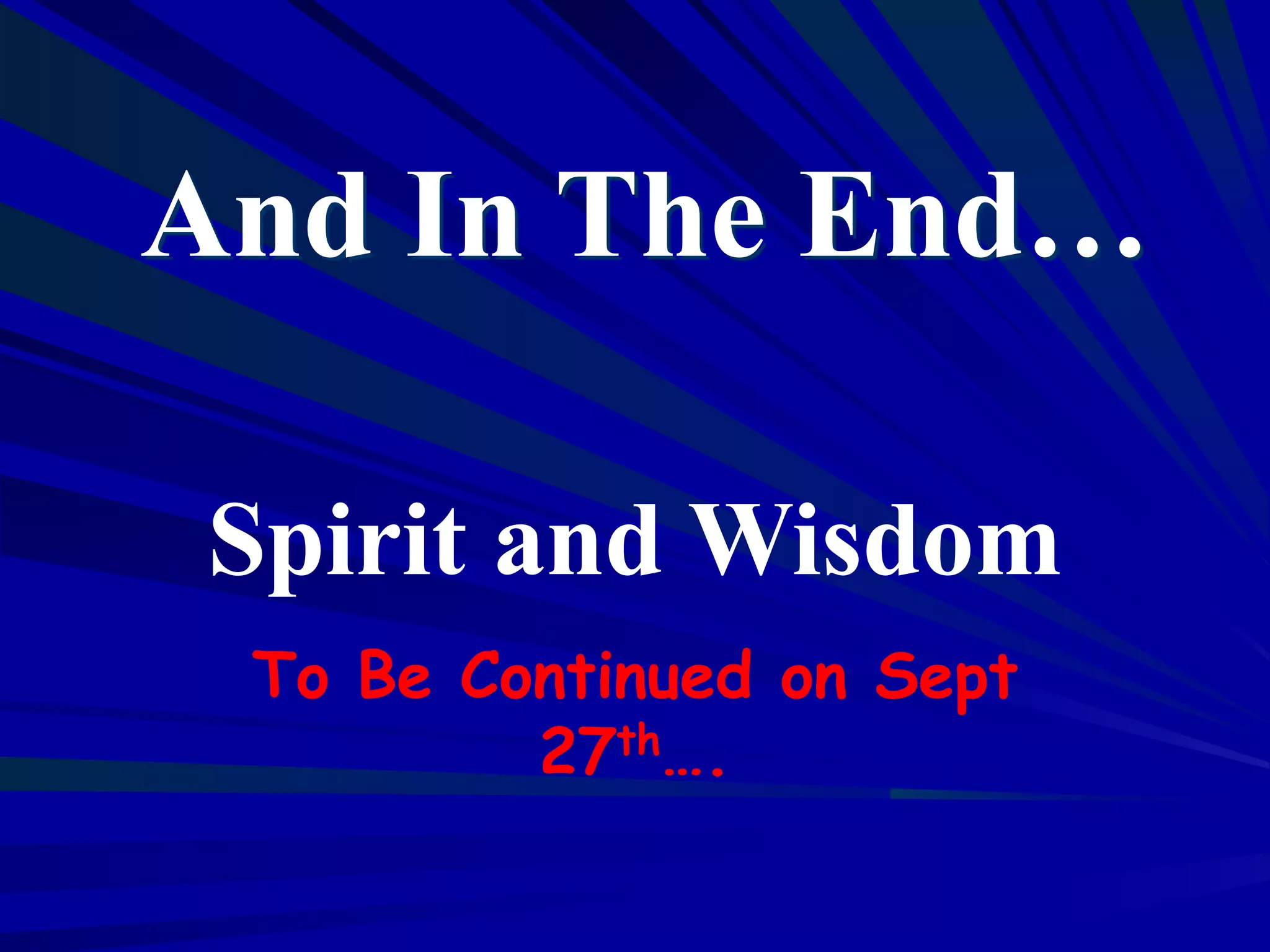
![Dependency Ratio: Retired/Working
1950 1960 1970 1980 1990 2000 2010 2020 2030 2040 2050
0
0.05
0.1
0.15
0.2
0.25
0.3
0.35
0.4
0.45
0.5
Dependency
Ratio
[Over
64]
/[20-65]
Year
Estimates Projections
Silver Tsunami](https://image.slidesharecdn.com/scalablebestpracticessmarthealth-131007195126-phpapp01/75/What-are-scal-able-best-prac-tices-to-spread-smart-health-8-2048.jpg)
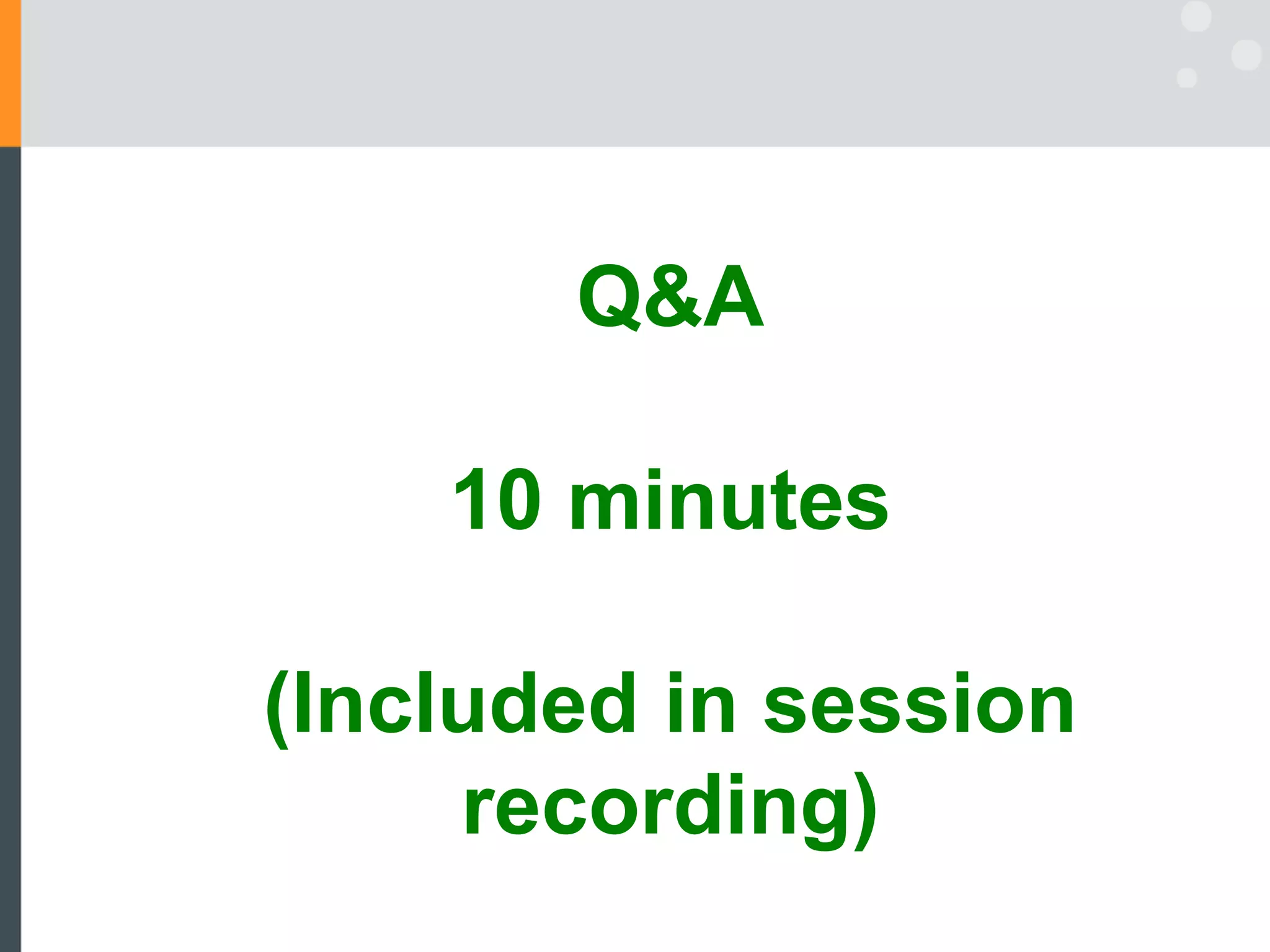
![Quality of Life over Life-Span
0 20 40 60 80 100 120
Age [Years]
Quality
of
Life
Rectangularization
after Fries, 1983
11](https://image.slidesharecdn.com/scalablebestpracticessmarthealth-131007195126-phpapp01/75/What-are-scal-able-best-prac-tices-to-spread-smart-health-11-2048.jpg)

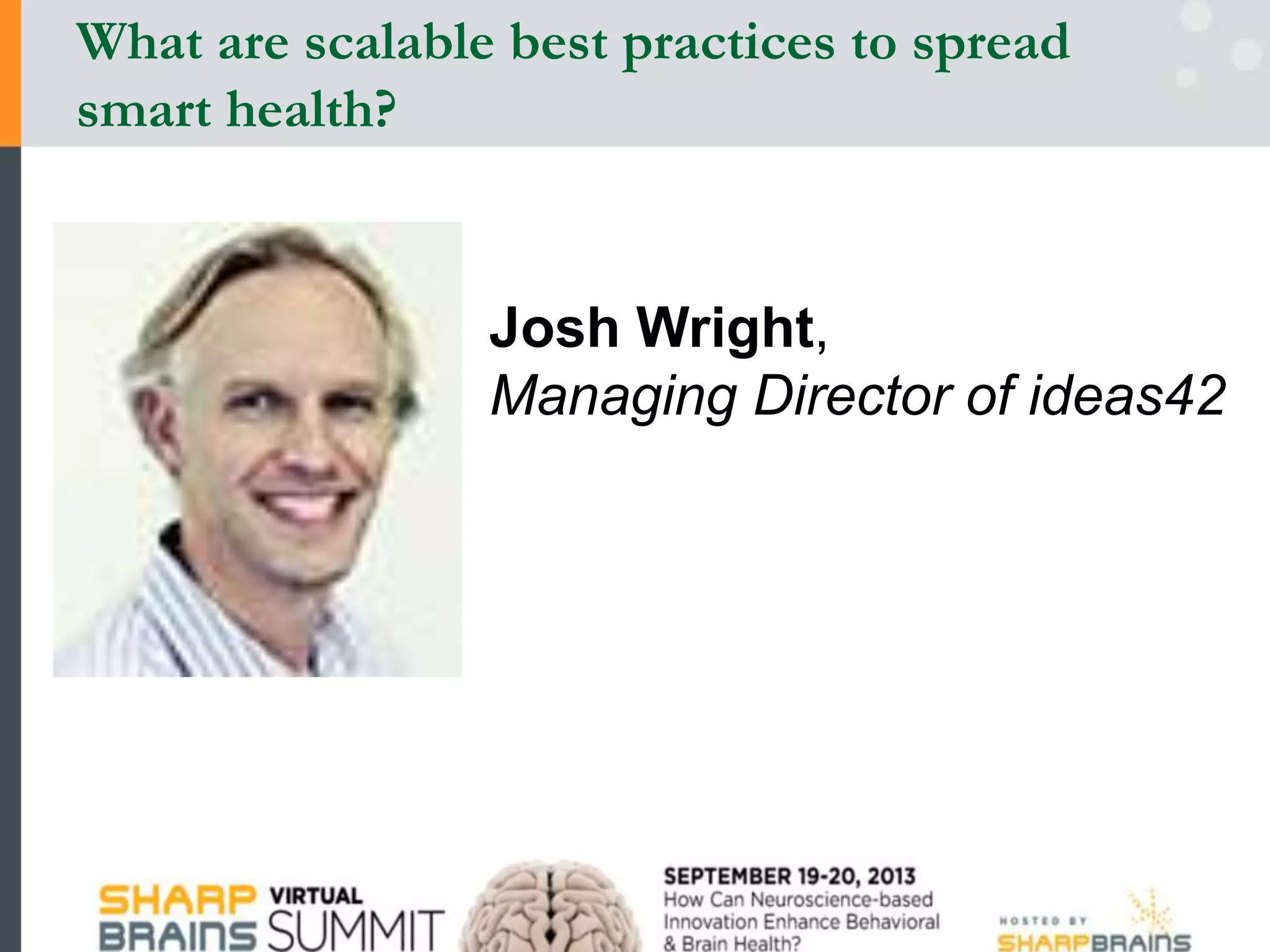
![Memory Model: Survival Analysis
36
0 5 10 15
0
0.5
1
Subject 1020, N = 8687
Probability
of
Correct
Intervening Number of Events
0 5 10 15 20 25
0
0.5
1
Probability
of
Correct
Intervening Time [sec]
1
b
t
a
M t F t e
](https://image.slidesharecdn.com/scalablebestpracticessmarthealth-131007195126-phpapp01/75/What-are-scal-able-best-prac-tices-to-spread-smart-health-36-2048.jpg)
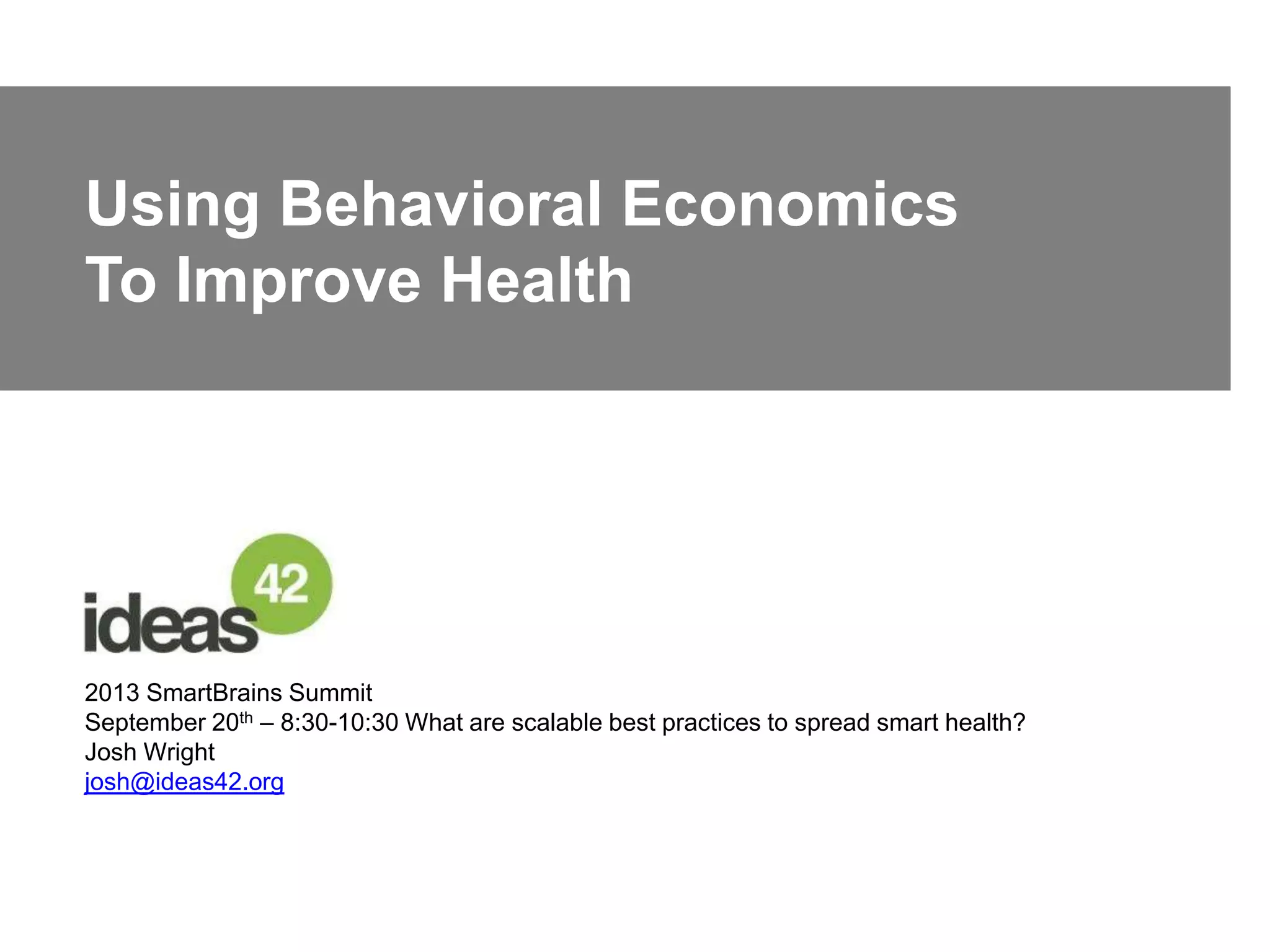
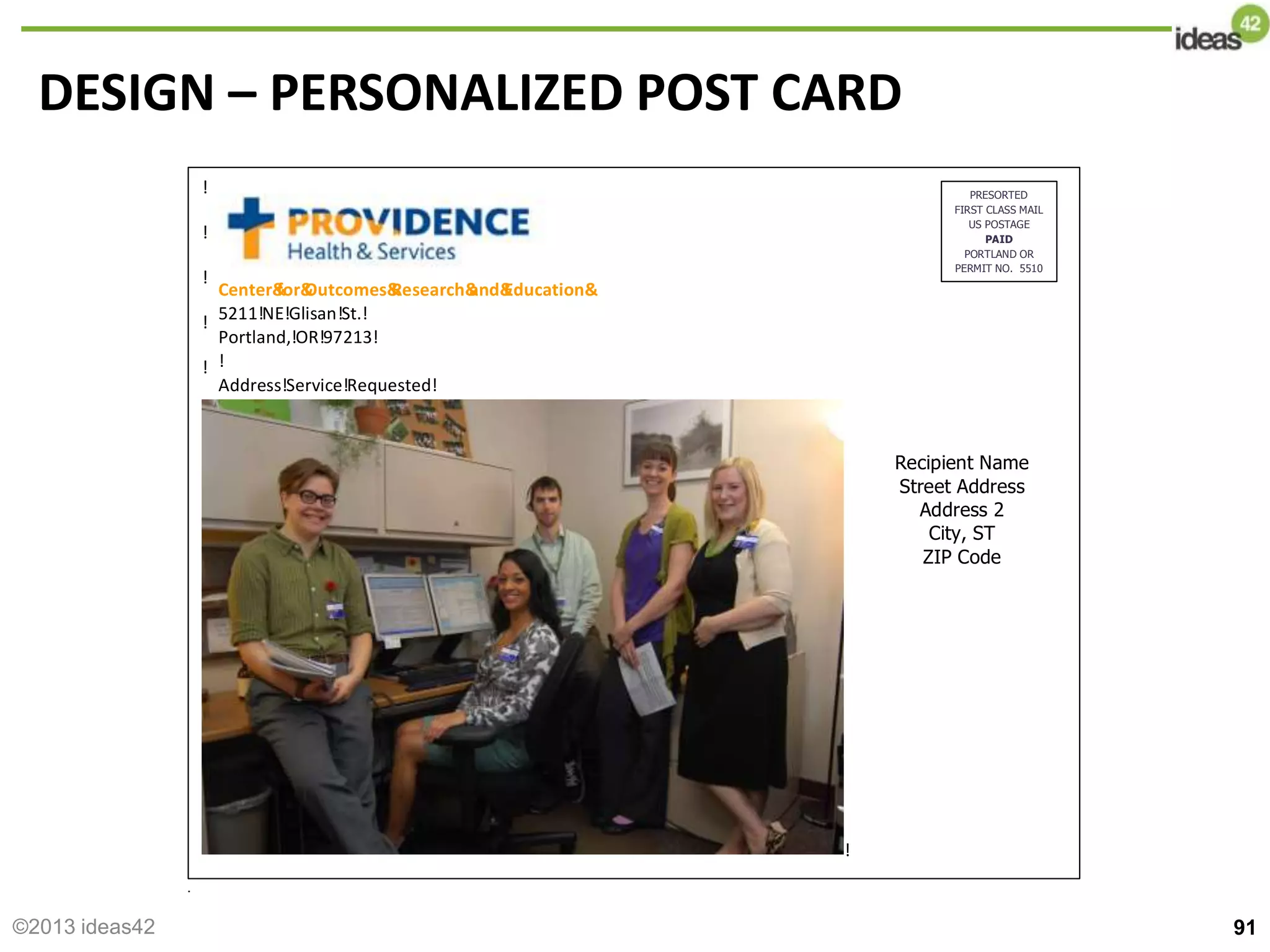
![92
before& &
You’ve'won'the'lottery'you'entered FREE&
HEALTH&
CARE Oregon&
Health&
Plan
Call&
toll&
free&
1=877=215=0686&
or&
email&
me&
at& 'with&
any&
questions—&
I&
am&
here&
to&
help!&
&
&
[RA&
circles&
photo&
and&
handwrites&
signature]
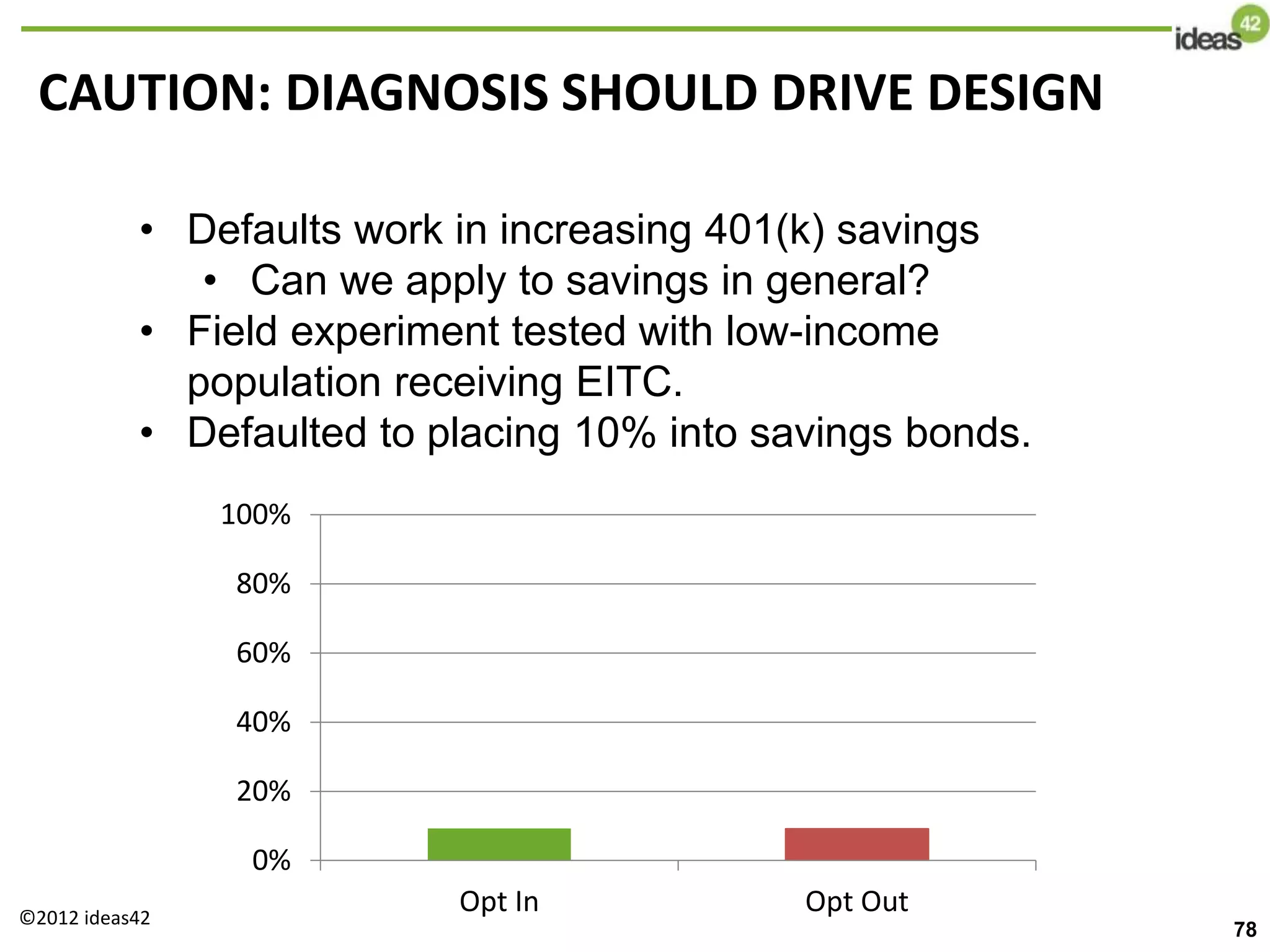
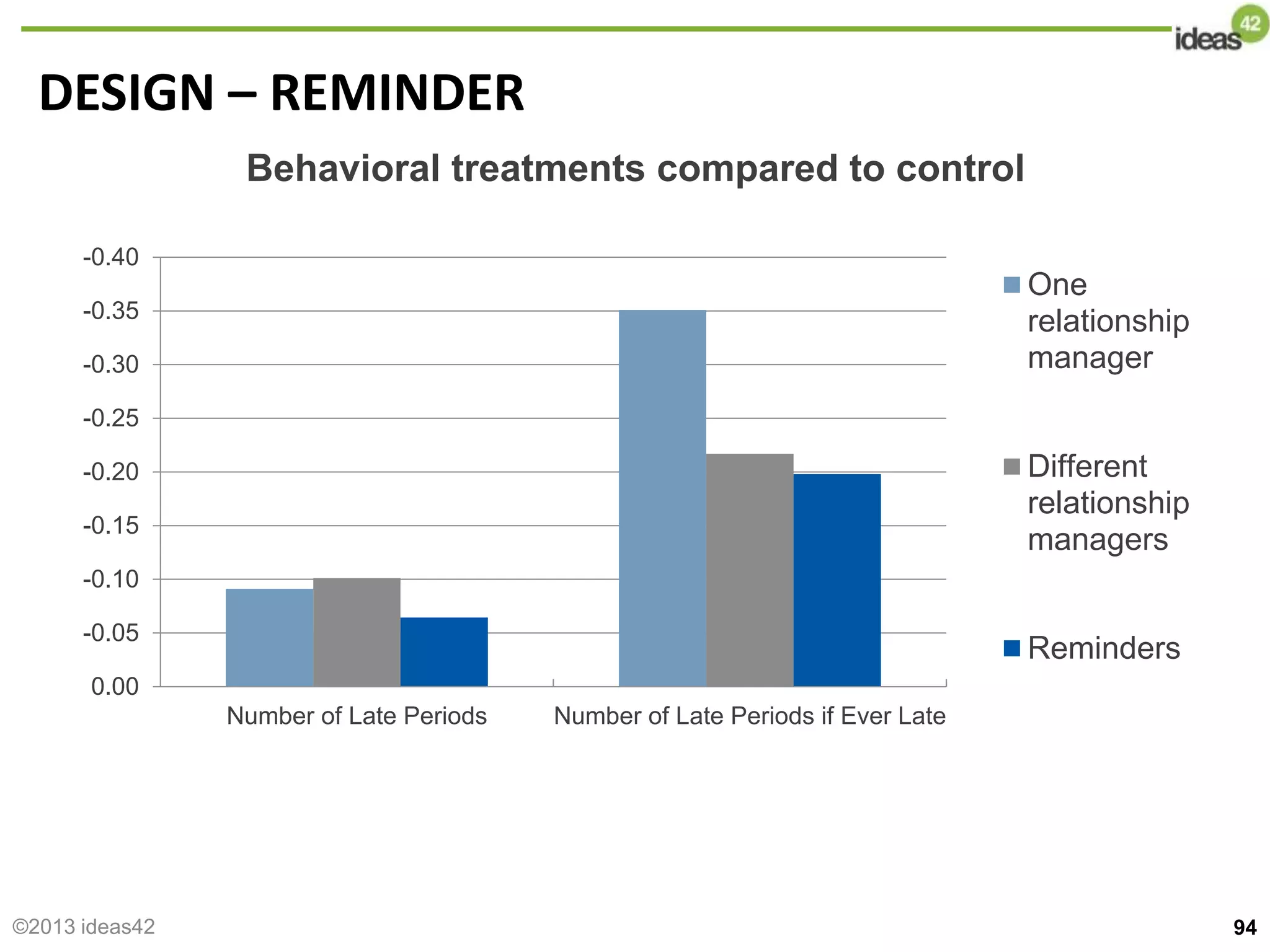
DESIGN – PERSONALIZED POST CARD
©2013 ideas42](https://image.slidesharecdn.com/scalablebestpracticessmarthealth-131007195126-phpapp01/75/What-are-scal-able-best-prac-tices-to-spread-smart-health-92-2048.jpg)


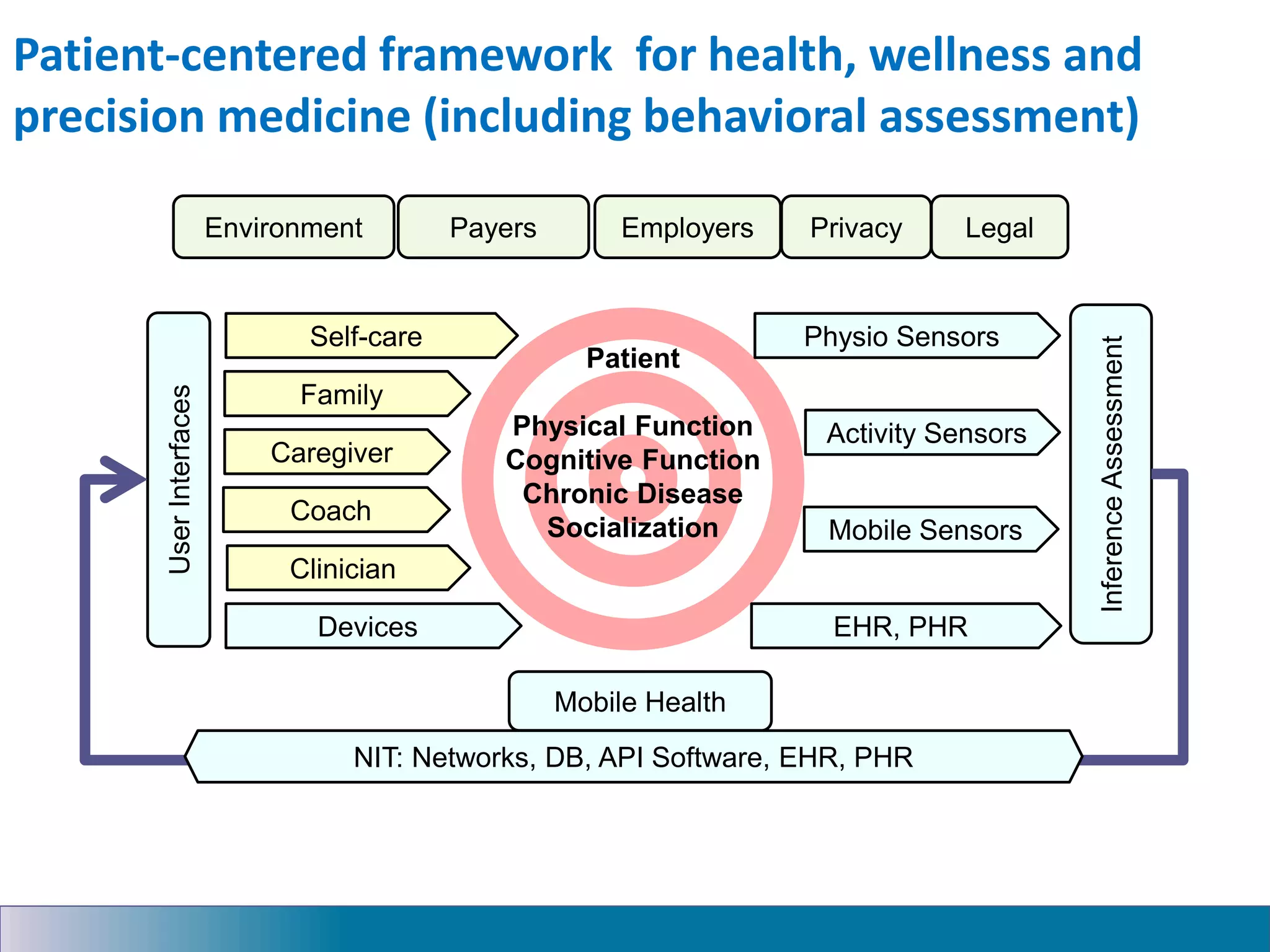
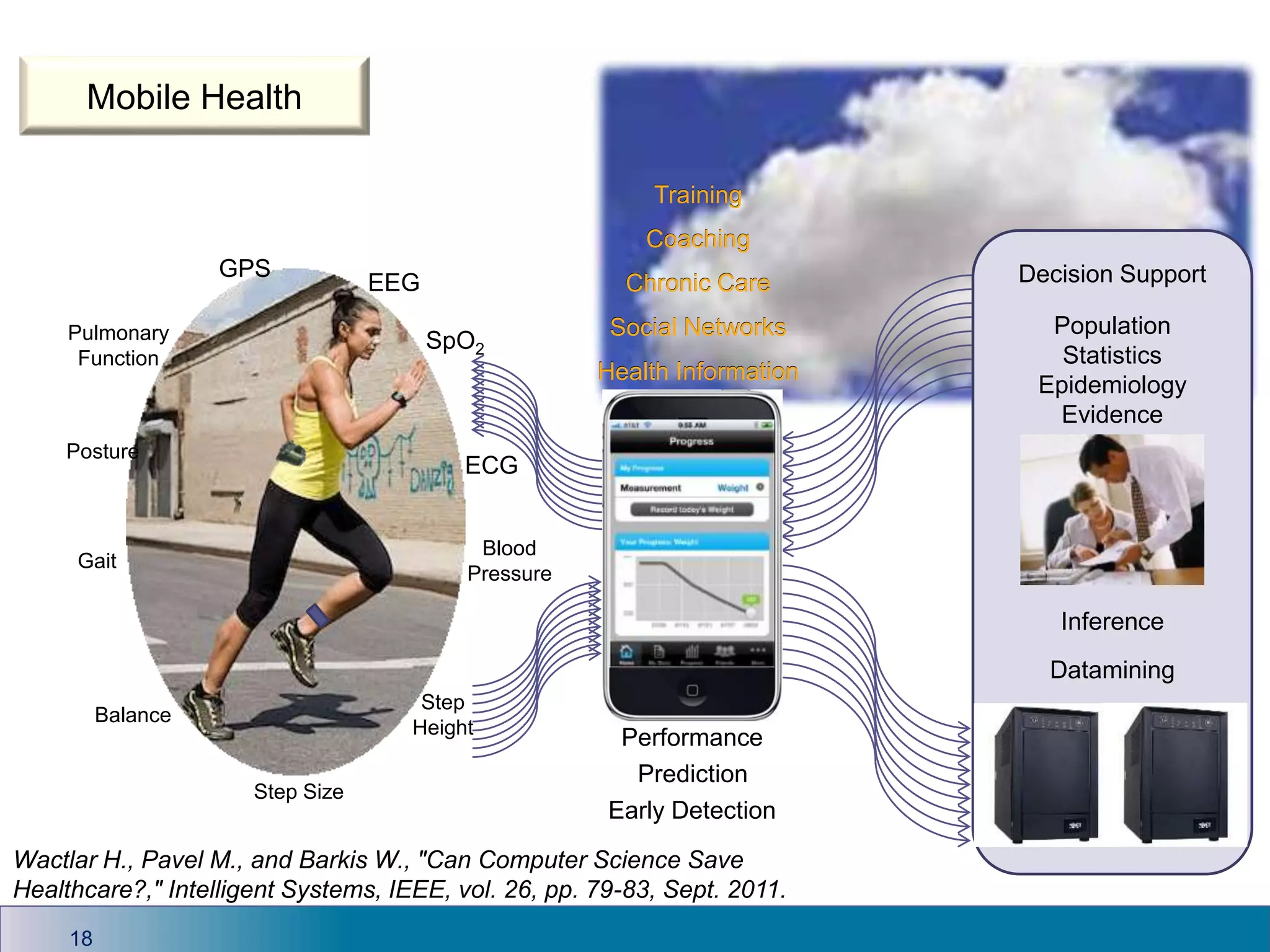
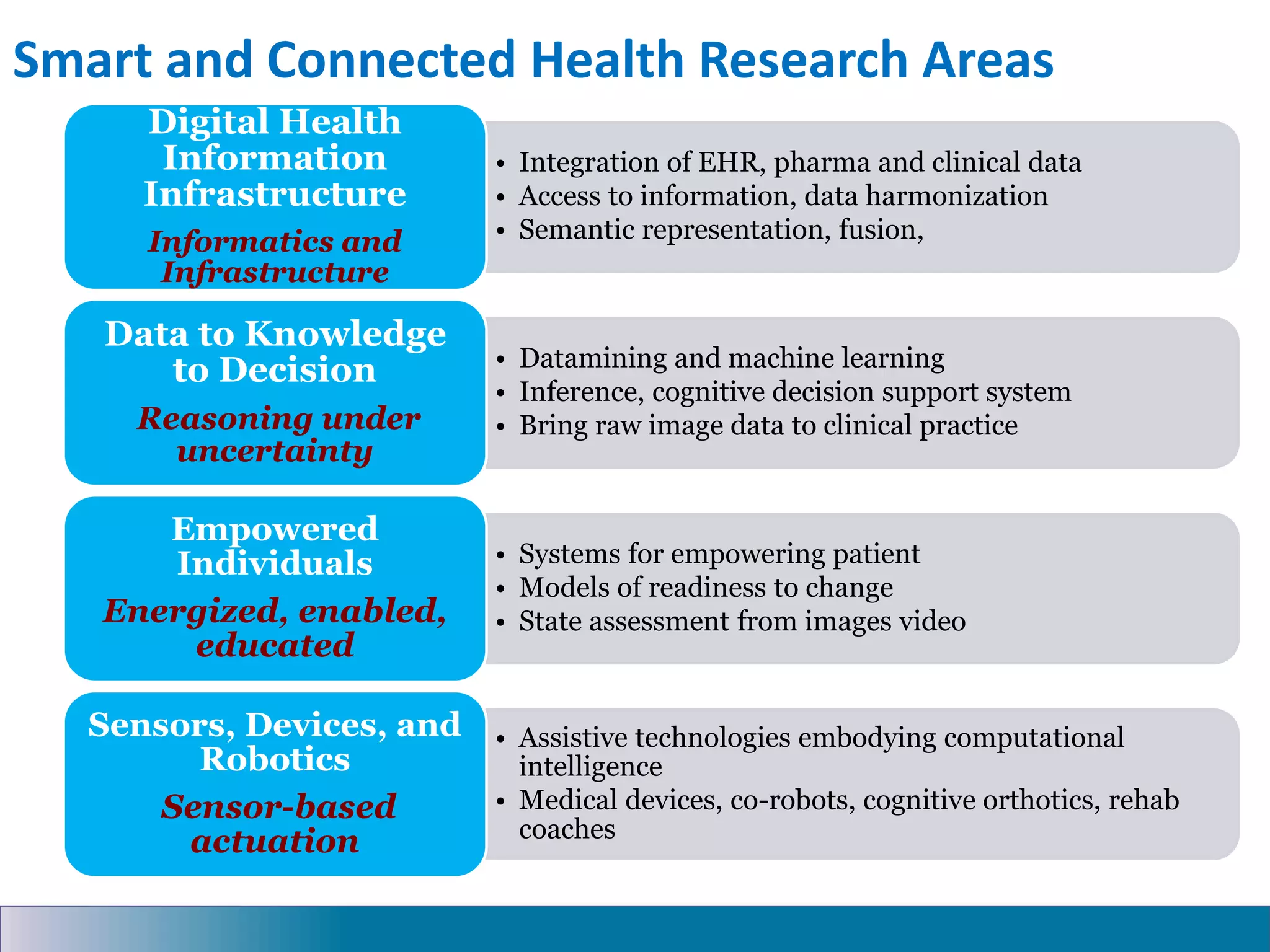
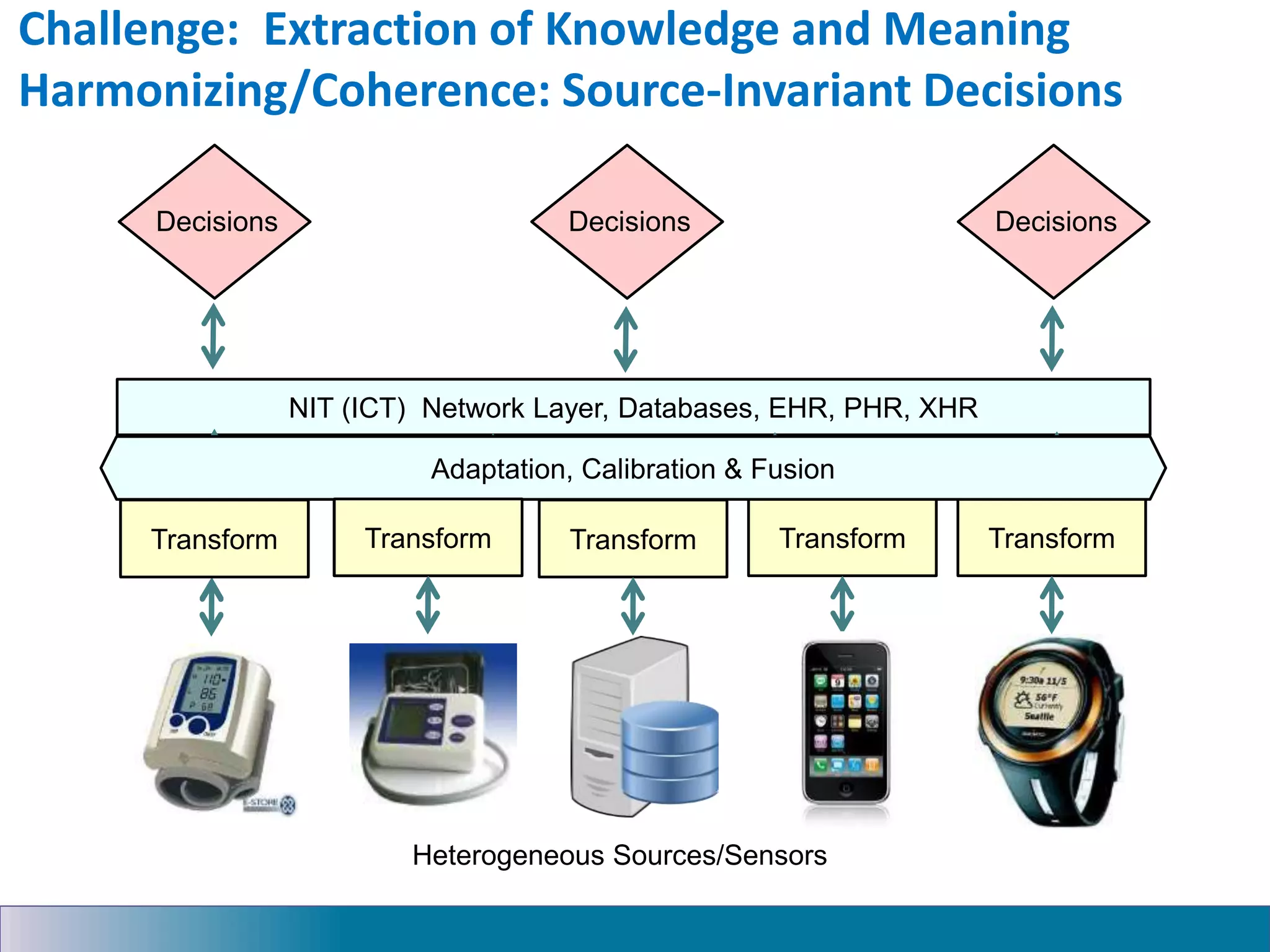
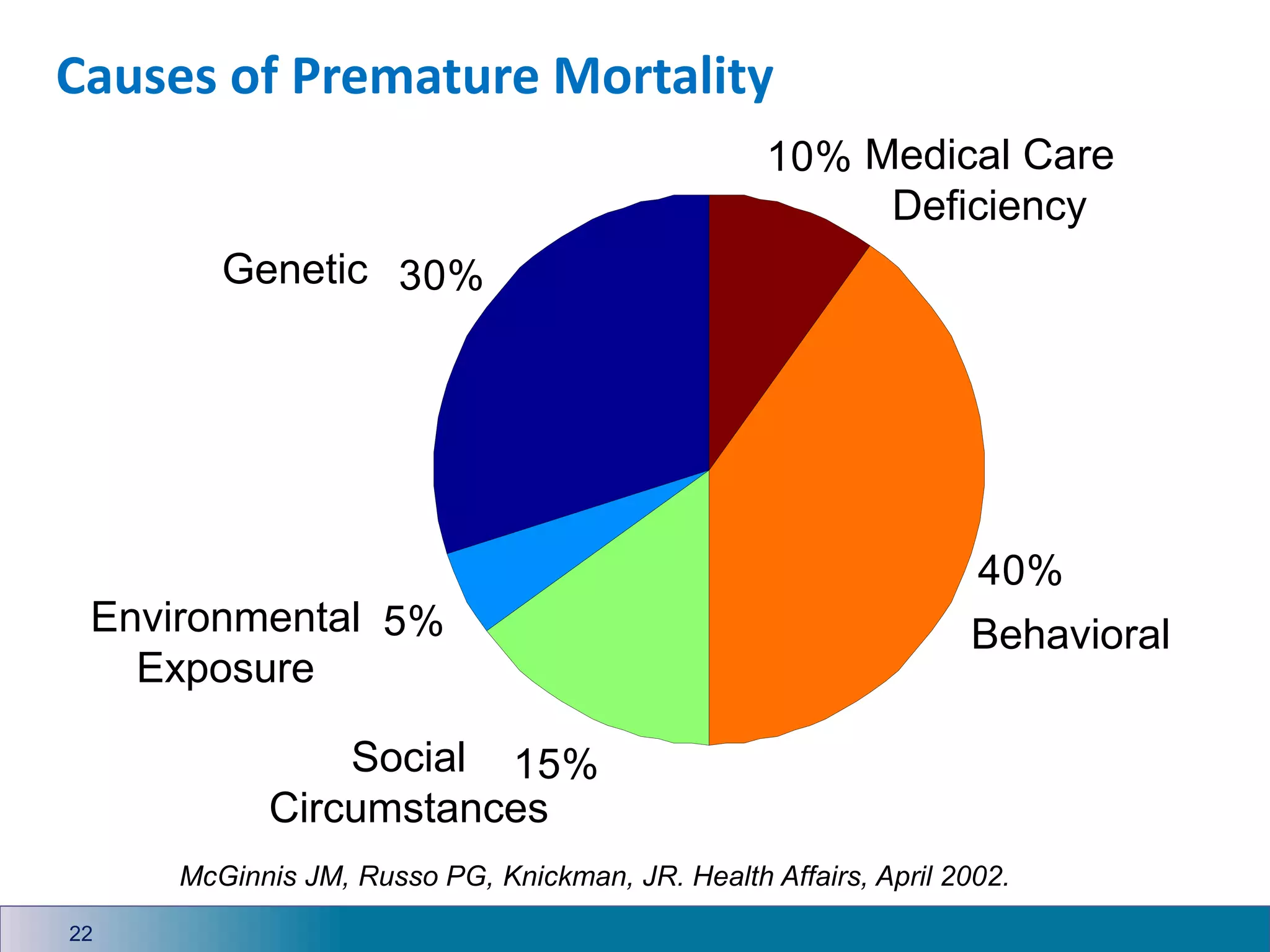
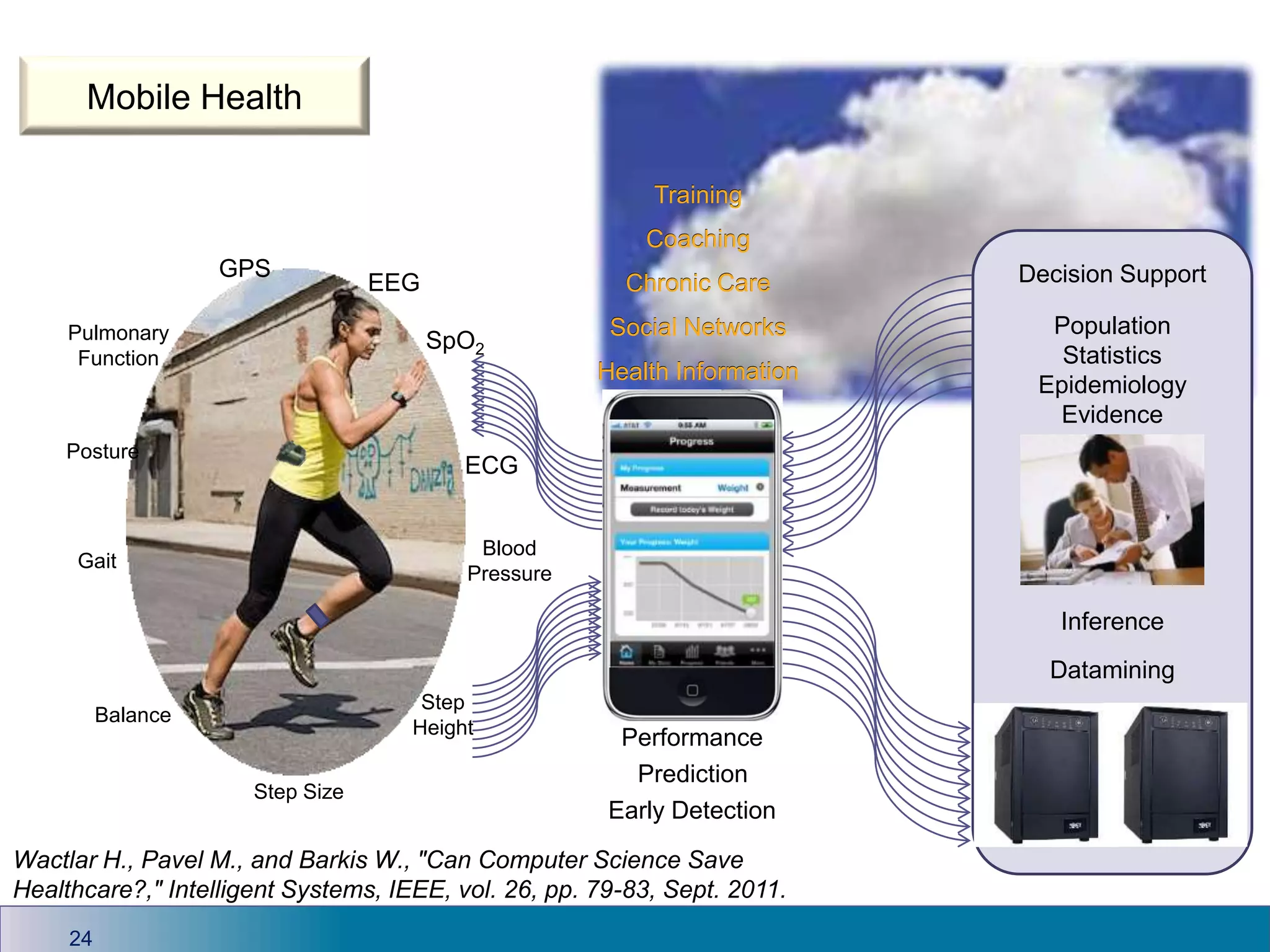
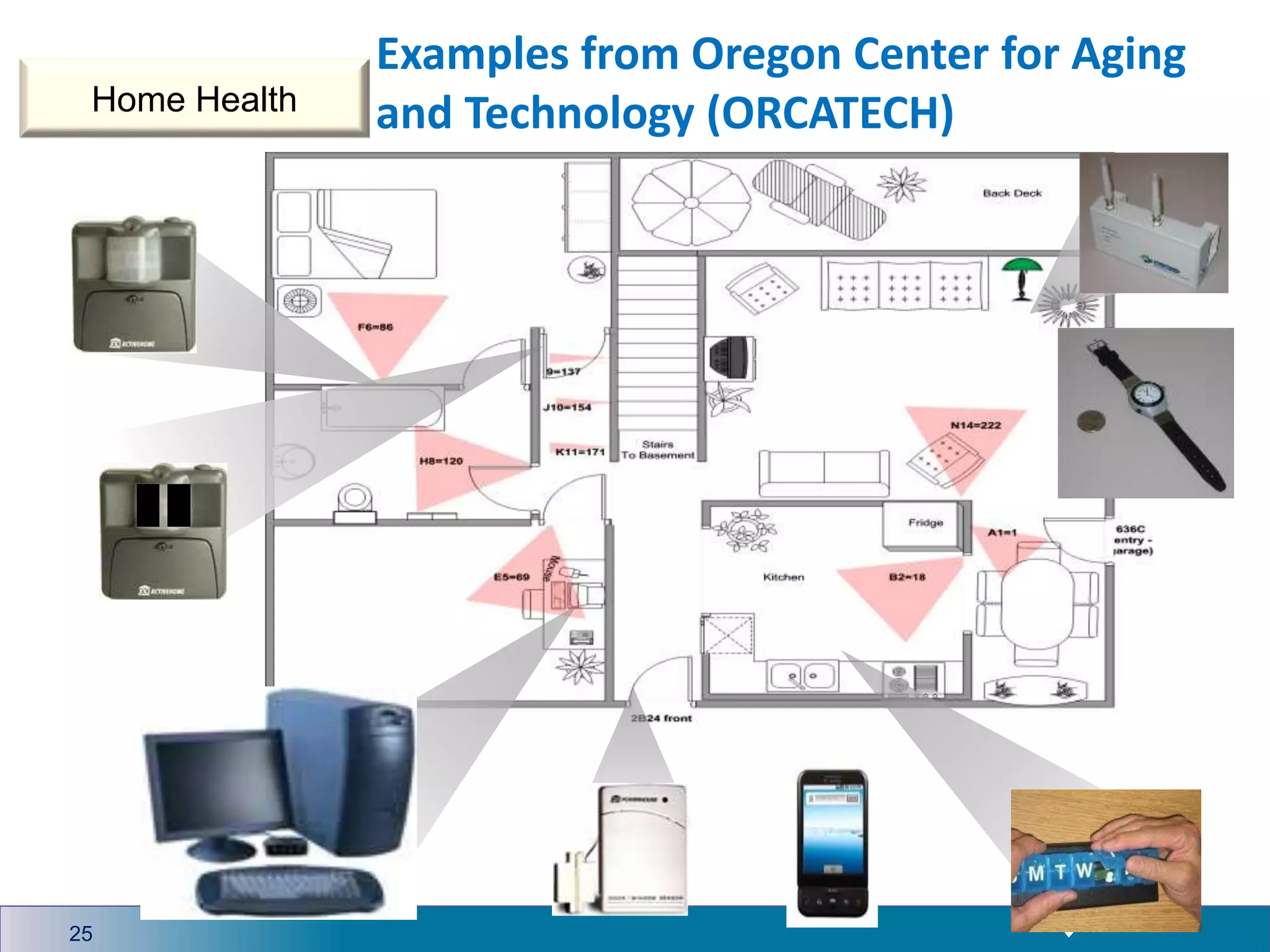
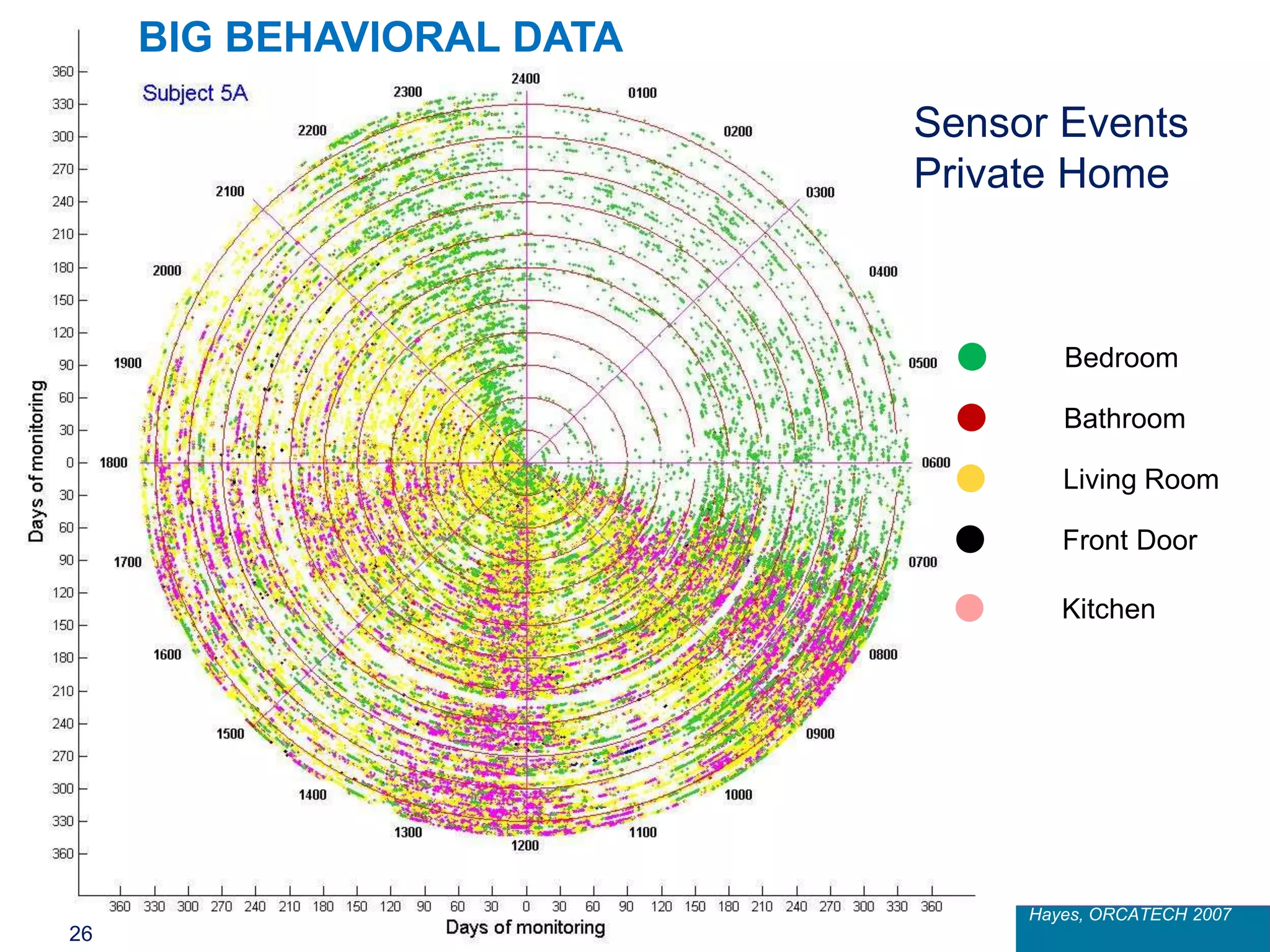
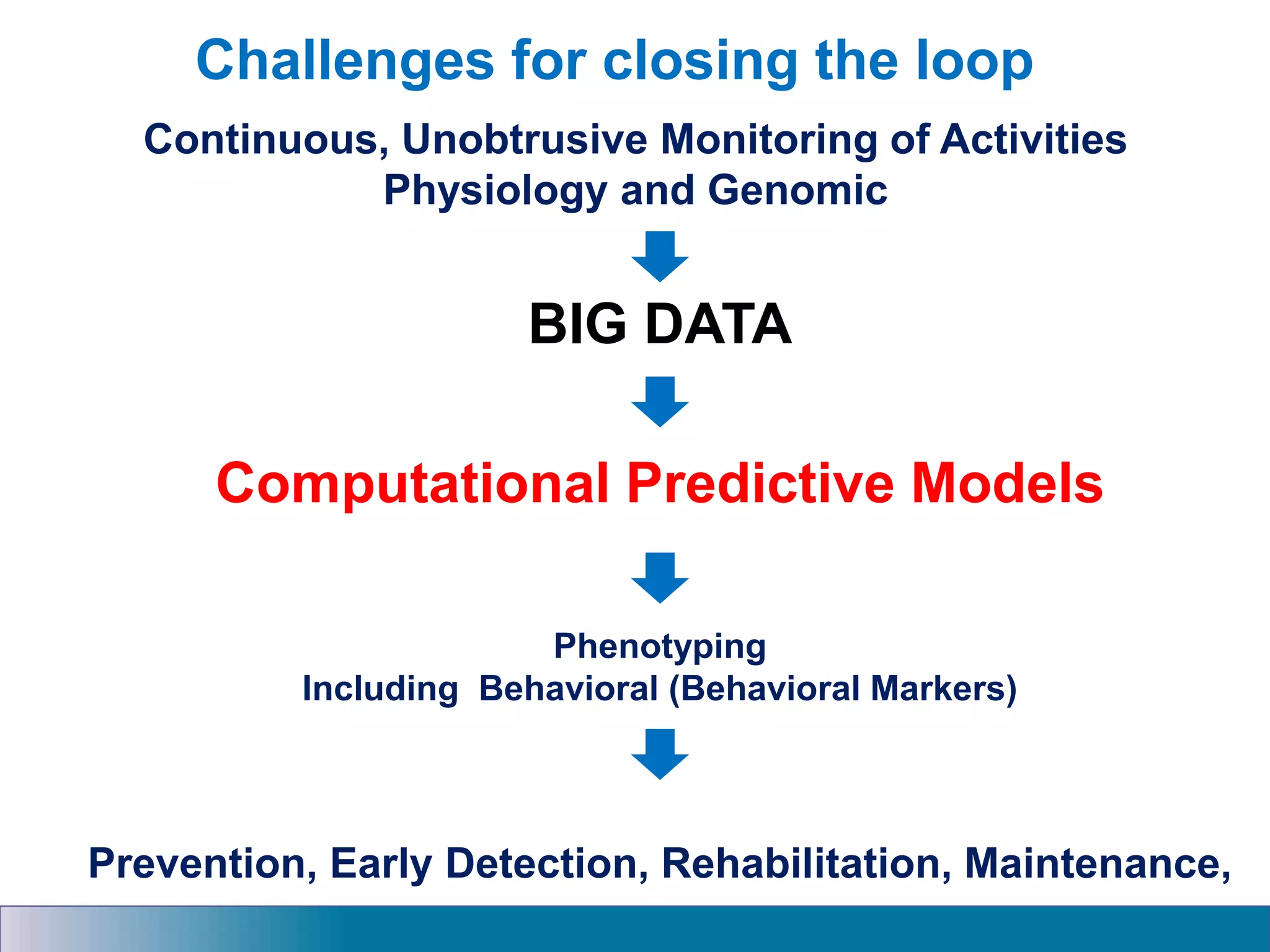
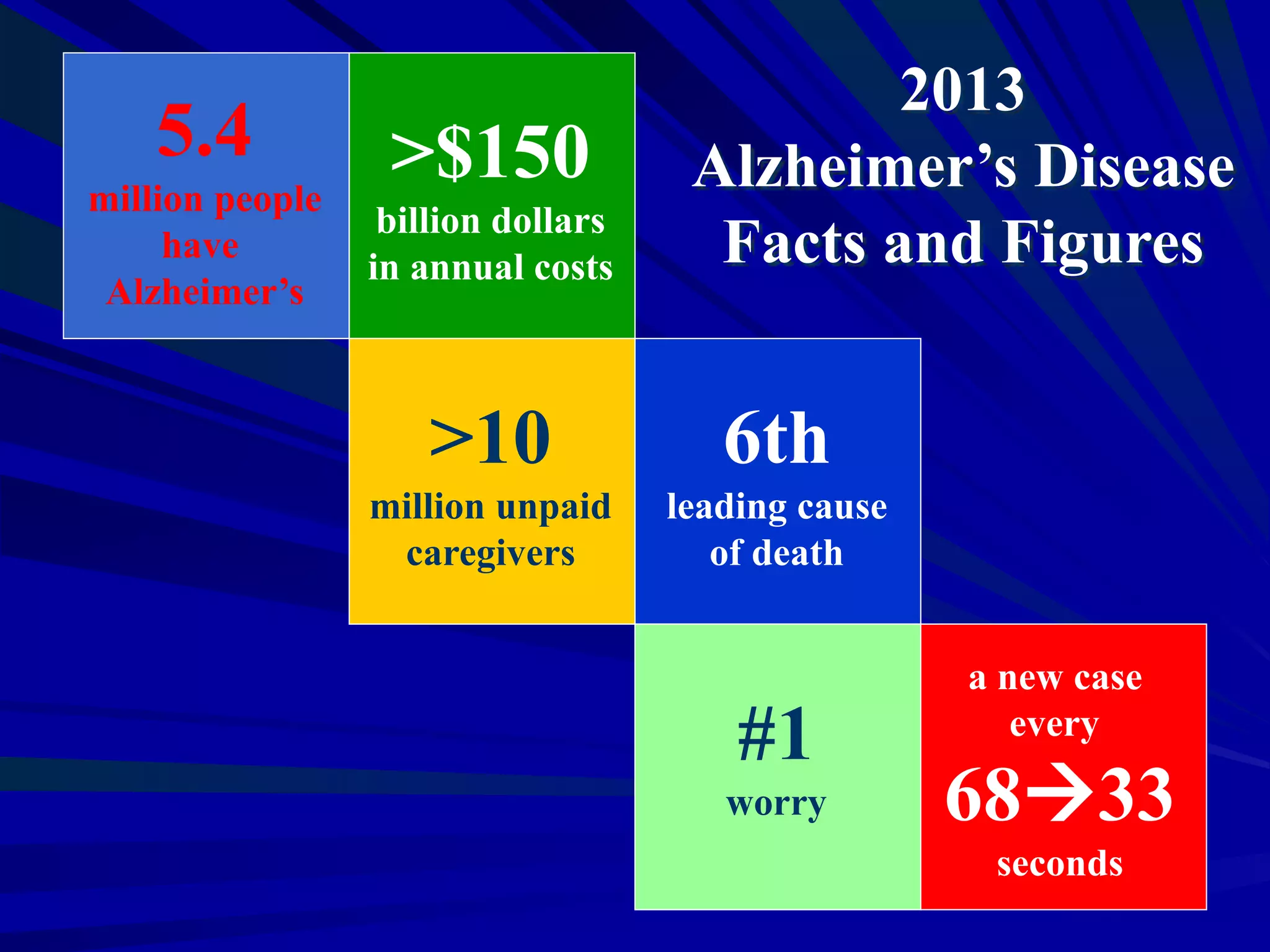
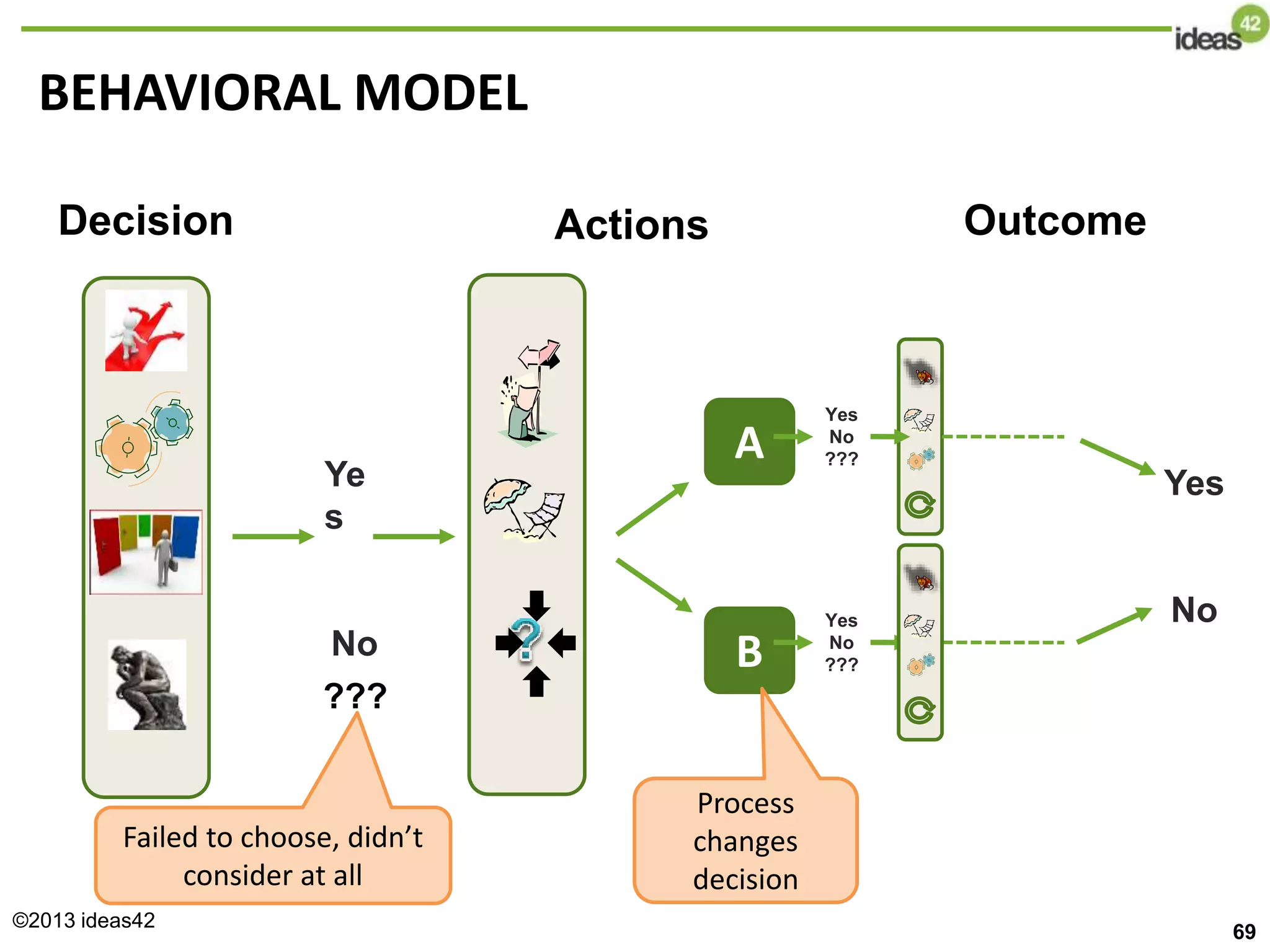
The document discusses the urgent need to innovate and implement scalable best practices for smart health, addressing the healthcare crisis in the U.S. with strategies focused on technology and behavior change. It highlights the Smart and Connected Health program objectives, aiming to improve health outcomes through integrated data and patient-centric approaches. Notably, it emphasizes the importance of addressing lifestyle factors in healthcare, particularly in the context of conditions like Alzheimer's disease.
































































































