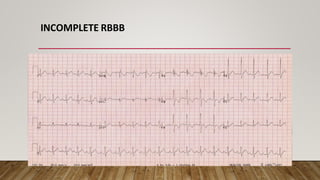
The document discusses Right Bundle Branch Block (RBBB), its types, diagnostic criteria, and underlying electrophysiological mechanisms. It explains the differences between complete and incomplete RBBB, focusing on QRS complex characteristics and associated ST segment and T wave changes. Additionally, it highlights various causes of RBBB and how anatomical factors contribute to conduction delays.