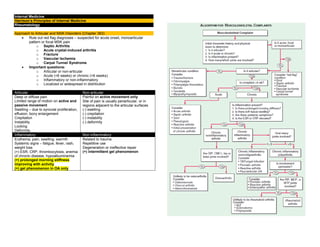
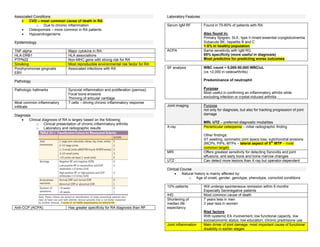
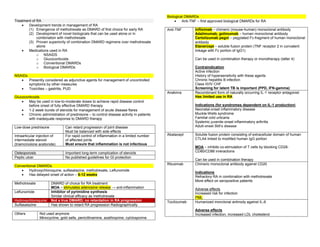
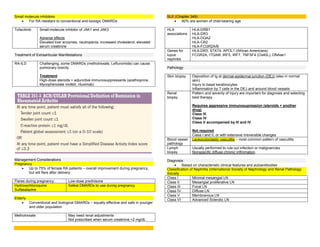
This document provides an overview of approaches to articular and musculoskeletal disorders, including osteoarthritis. It discusses evaluating patients for red flag diagnoses like infection or fracture. Key factors to determine include if the pain is articular or non-articular, acute or chronic, inflammatory or non-inflammatory. Risk factors for osteoarthritis include age, obesity, injury, and joint alignment. Symptoms include joint pain and stiffness. Treatment involves exercise, weight loss, bracing, acetaminophen, NSAIDs, and surgery for advanced cases.