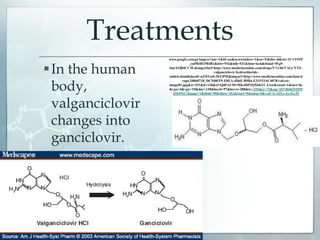
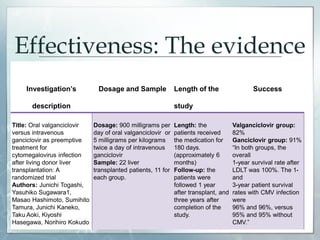
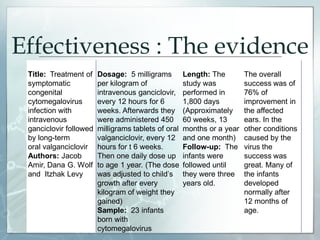
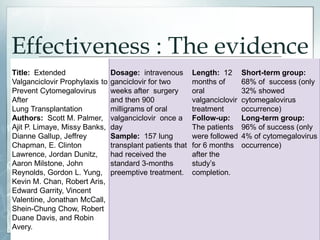
This document discusses whether valganciclovir is the best preventive treatment for cytomegalovirus (CMV). It begins by introducing CMV as a herpes virus that infects over 80% of adults without symptoms. The document then reviews several studies that tested valganciclovir or ganciclovir treatments in transplant patients and infants. The studies found success rates from 68-96% depending on dosage and duration. The document concludes that valganciclovir is superior to other approved treatments and that combining intravenous then oral medications provides the best prevention and treatment of CMV.

![References
Amir J, Levy I, Wolf DG. 2010. Treatment of symptomatic congenital
cytomegalovirus infection with intravenous ganciclovir followed by long-term
oral valganciclovir. European Journal of Pediatrics [Internet]; [revised 201 January
13; Cited: 2012 October 19]. DOI 10.1007/s00431-010-1176-9:1061–1067. Available
at: http://www.springerlink.com/content/bg650327335h16r0/fulltext.html
Aoki T, Hasegawa K, Hashimoto M, Kaneko J, Kokudo N, Sugawara Y, Tamura
S, Togashi J. 2011. Oral valganciclovir versus intravenous ganciclovir as
preemptive treatment for cytomegalovirus infection after living donor liver
transplantation: A randomized trial. BioScience Trends [Internet]; [revised 2011
September 26; Cited: 2012 October 12].DOI:10.5582/bst.2011.v5.5.217:217-222.
Available at:
http://web.ebscohost.com.uprcdb.cayey.upr.edu:2048/ehost/pdfviewer/pdfvie
wer?sid=f754d515-ff02-48c5-a7be-
ba0eea36253a%40sessionmgr112&vid=5&hid=106](https://image.slidesharecdn.com/reviewpaperpresentation-130531110223-phpapp02/85/Review-paper-presentation-19-320.jpg)
![References
Aris R, Avery R, Banks M, Chan KM, Chapman J, Chow S-C, Davis
RD, Dunitz J, Gallup D, Garrity E, Lawrence EC, Limaye AP, McCall J,
Milstone A, Palmer SM, Reynolds J, Valentine V, Yung GL. 2010.
Extended Valganciclovir Prophylaxis to Prevent Cytomegalovirus
After Lung Transplantation: A Randomized, Controlled Trial. Annals
of Internal Medicine. [Internet]; [Cited: 2012 November 1].
152(12):761-769. Available at:
http://annals.org/article.aspx?articleid=745830
Biron KK. 2006. Antiviral drugs for cytomegalovirus diseases.
Elsevier. [Internet]; [Cited: 2012 November 20]. 71:154–163.
doi:10.1016/j.antiviral.2006.05.002 Available at:
http://www.idpublications.com/journals/pdfs/avres/avres_mostcit
ed_1.pdf](https://image.slidesharecdn.com/reviewpaperpresentation-130531110223-phpapp02/85/Review-paper-presentation-20-320.jpg)
![References
Bloom RD, Blumberg E, Trofe-Clark J, Wade Ticehurst E. 2010. Valganciclovir for
the prophylaxis and treatment of cytomegalovirus infection in solid organ
transplantation. Transplant Research and Risk Management. [Internet]; [Cited: 2012
November 18]. 2010(2): 29-39. DOI:http://dx.doi.org/10.2147/TRRMS5979
Available at: http://www.dovepress.com/valganciclovir-for-the-prophylaxis-and-
treatment-of-cytomegalovirus-in-peer-reviewed-article-TRRM
Christiansen CB, Cunha-Bang C, Fox ZV, Hillings JG, Iversen M, Kirkby NS,
Lundgren JD, Mortensen SA, Rasmussen A, Sengel VH, Sorensen SS. 2010. Factors
associated with the development of cytomegalovirus infection following solid organ
transplantation. Scandinavian Journal of Infectious Diseases. [Internet]; [Cited: 2012
December 7]. 43: 360–365. DOI: 10.3109/00365548.2010.549836. Available at:
http://web.ebscohost.com.uprcdb.cayey.upr.edu:2048/ehost/pdfviewer/pdfviewer?sid
=f8f3123a-7b4c-4229-9c76-6163b0175560%40sessionmgr114&vid=1&hid=104](https://image.slidesharecdn.com/reviewpaperpresentation-130531110223-phpapp02/85/Review-paper-presentation-21-320.jpg)
![References
Garofoli F, Lombardi G, Stronati M. 2010. Congenital cytomegalovirus infection:
treatment, sequelae and follow-up. The Journal of Maternal-Fetal and Neonatal
Medicine. [Internet]; [Cited: 2012 December 7]. 23: 45–48. DOI:
10.3109/14767058.2010.506753. . Available at:
http://web.ebscohost.com.uprcdb.cayey.upr.edu:2048/ehost/pdfviewer/pdfviewer?sid=b
ad51aef-4205-481d-a6a0-a3970a1cd335%40sessionmgr113&vid=1&hid=104
Goodheart CR. 1969. An Introduction to Virology. Chicago (Illinois): W.B.
Saunders Company. What is a Virus?; p 364
Goodheart CR. 1969. An Introduction to Virology. Chicago (Illinois): W.B.
Saunders Company. Tumor Viruses that contain DNA; p 334-336.
Razonable RR and Emery VC. 2004. Management of CMV infection and
disease in transplant patients. Management Recommendations. 11: 77–86](https://image.slidesharecdn.com/reviewpaperpresentation-130531110223-phpapp02/85/Review-paper-presentation-22-320.jpg)