This document provides an overview of retinoids, including:
- Retinoids are derivatives of vitamin A or compounds with similar structure or function to vitamin A.
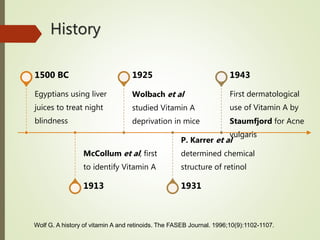
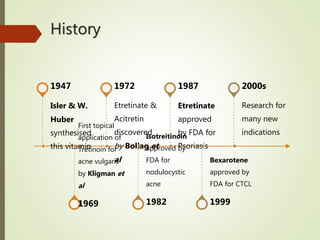
- They have a long history of medical use dating back to ancient Egypt.
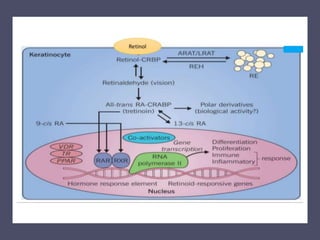
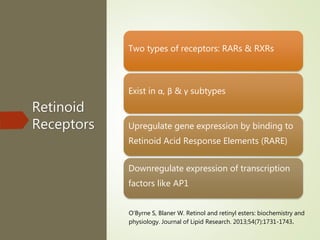
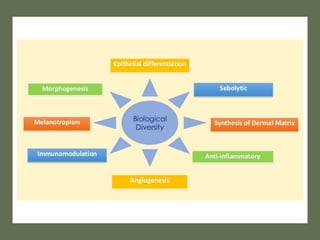
- Retinoids act through nuclear retinoid receptors and influence gene expression and cell differentiation.
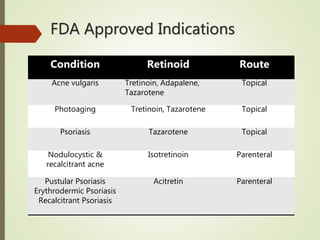
- They have various applications in dermatology for conditions like acne and psoriasis, ophthalmology for preventing blindness, and oncology for treating cancers like cutaneous T-cell lymphoma.
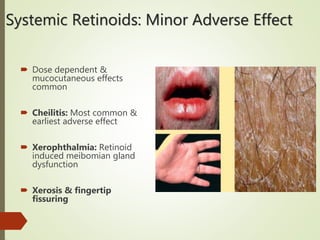
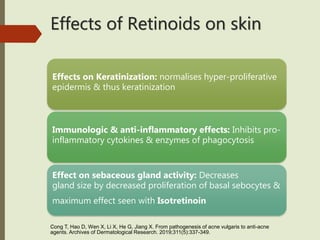
- Both topical and oral retinoids are used depending on the condition, and they can have beneficial effects as well as potential adverse side effects that require monitoring.

![Classification
First Generation: Non-aromatic
naturally occurring retinoids: retinol,
retinal, isotretinoin & alitretinoin
Second generation: Monoaromatic
lipophilic compounds: Etretinate,
Acitretin, Motretinate
Third generation: Cyclised polyene
side chain compounds: Adapalene,
Tazarotene & Bexarotene
Goodman L, Gilman A, Brunton L, Hilal-Dandan R, Knollmann B.
Goodman & Gilman's the pharmacological basis of therapeutics. 13th
ed. New York [etc.]: McGraw Hill Education; 2018.](https://image.slidesharecdn.com/retinoidsintherapy-190611100611/85/Retinoids-in-therapy-5-320.jpg)
![National
Vitamin A
Prophylaxis
Programme
Five year trial by NIN: Massive dose of Vit A
(200000 IU) administered per 6 months between 1
& 3 years reduces corneal xerophthalmia by 80%
1970: National Prophylaxis Programme Against
Nutritional Blindness
2006: Age group broadened; 6 months-5 years
Dose: 100000 IU at 9 months followed by 200000
IU, 6 monthly up to 5 years
National Vitamin A prophylaxis program | National Health Portal Of India
[Internet]. Nhp.gov.in. 2019 [cited 6 June 2019]. Available from:
https://www.nhp.gov.in/national-vitamin-a-prophylaxis-program_pg](https://image.slidesharecdn.com/retinoidsintherapy-190611100611/85/Retinoids-in-therapy-33-320.jpg)