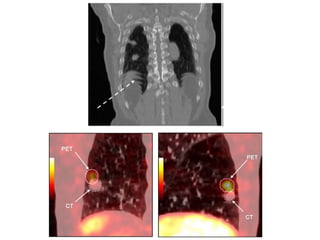
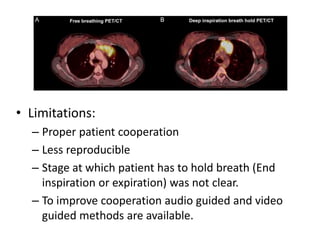
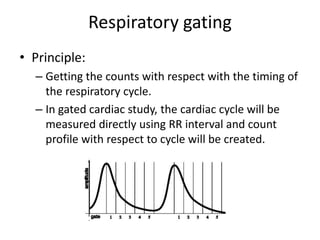
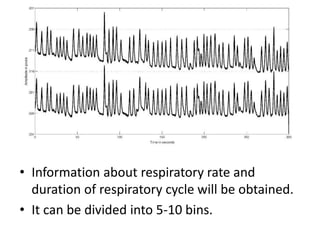
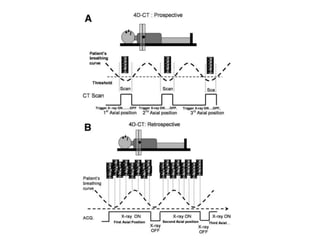
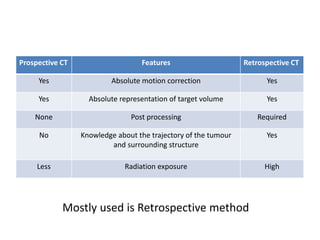
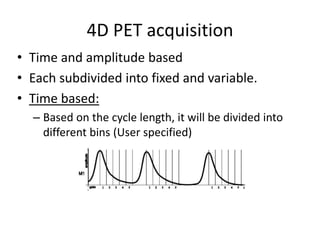
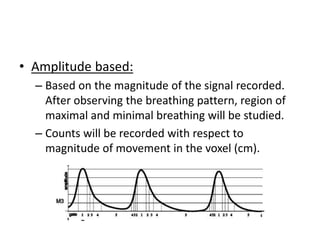
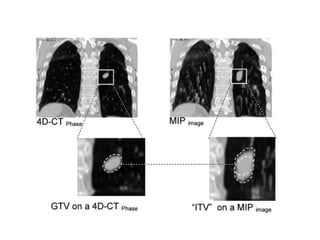
Respiratory gating is needed to accurately delineate tumor volume affected by respiration. Two main methods are respiratory gating and deep inspiratory breath hold (DIBH). Respiratory gating uses external monitors like optoelectric or pressure methods to track respiration and bin PET/CT data. 4D CT can be prospective or retrospective, with retrospective preferred. 4D PET data is binned by time or amplitude. Data is processed as MIP, AVE or summed images, with summed preferred for PET. Limitations include longer scan time and potential patient discomfort from irregular breathing.







































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

