Introduction Of RenalFunction
Kidneys help maintain homeostasis by excreting
waste products, regulating fluid balance, and
producing hormones (erythropoietin, renin,
calcitriol).
Tip:- (erythropoietin is a hormone that stimulates
red blood cell production, renin is an enzyme that
initiates the renin-angiotensin-aldosterone system
to regulate blood pressure, and calcitriol is the
active form of Vitamin D that promotes calcium
absorption for bone health)
3.
Continue.......
Tests detect kidneyabnormalities early
and monitor renal disease progression.
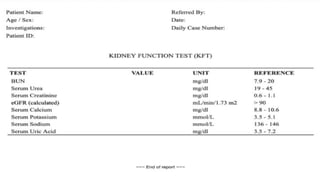
A Renal Function Test (RFT), or
Kidney Function Test (KFT), is a group
of blood and urine tests to assess
kidney health and function.
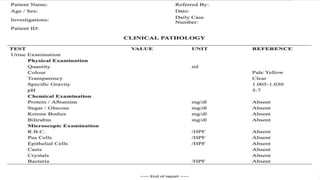
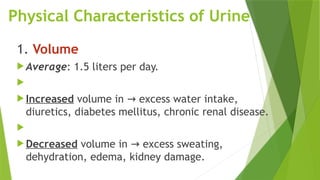
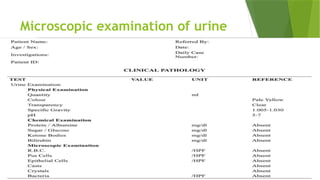
Examination of Urine
Physicaland Chemical Examination
In clinical biochemistry, urine is tested and report is given on a
urine sample. The procedure is called urine analysis .
If the kidneys are not functioning properly, waste products can
accumulate in the blood, and fluid levels can increase to
dangerous volumes, causing damage to the body or a potentially
life-threatening situation.
Numerous conditions and diseases can result in damage to the
kidneys.
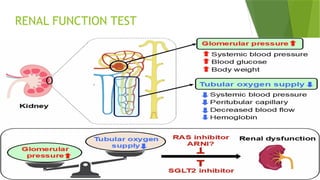
1. Glomerular FunctionTests
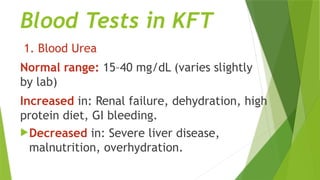
These test how well the kidneys filter waste products.
Blood Urea – Measures urea levels in blood (high in renal failure).
Serum Creatinine – More reliable than urea for kidney function.
Clearance Tests
Inulin clearance – Gold standard for Glomerular Filtration Rate
(GFR).
Creatinine clearance – Commonly used to estimate GFR.
Urea clearance – Less accurate, sometimes used.
8.
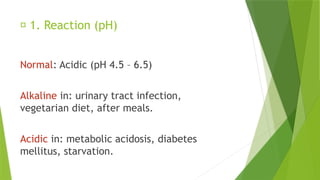
🔹 2. TubularFunction Tests
These check the kidney tubules’ ability to concentrate and dilute urine,
and maintain acid-base balance.
concentration test – After water restriction, kidneys should concentrate
urine.
Urine dilution test – After excess water intake, kidneys should dilute
urine.
Acidification test – Measures kidney’s ability to excrete hydrogen ions.
Phenolsulfonphthalein (PSP) test – Old test, measures tubular excretion
function.
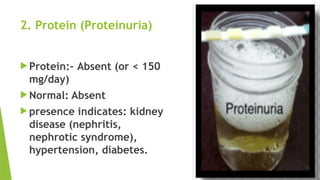
Proteins in urine – Presence indicates tubular/glomerular damage.
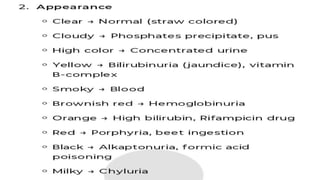
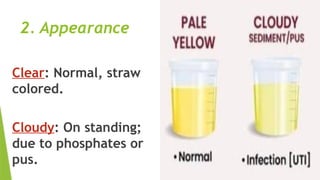
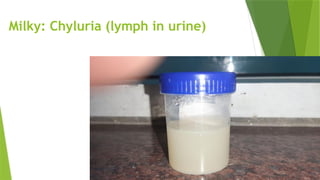
Chyluria is arare condition where
chyle (lymph and fats from the
intestines) leaks into the urinary
tract, causing urine to appear
milky white. It is primarily caused
by parasitic infections,
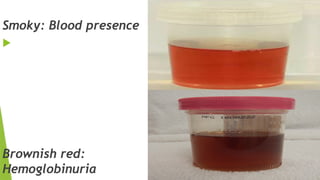
Blood in Urine
HematuriaSeen in nephritis and postrenal
→
hemorrhage.
Hemoglobinuria Due to abnormal hemolysis.
→
Tests available: Hemastix strips (rapid detection).
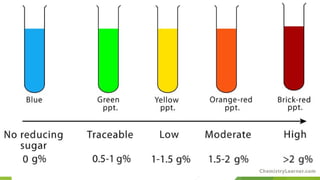
Reducing Sugars (Glycosuria)
(presence of glucose in urine)
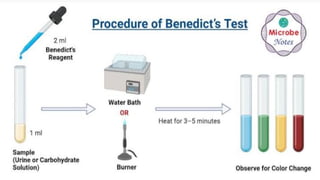
Benedict’s test: Used to know % of reducing sugars
in urine.
Procedure:
Take ~1 mL Benedict’s reagent in a test tube.
Add 4–5 drops of urine sample.
Heat to boiling.
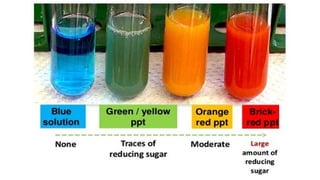
Positive test → reddish-brown (orange, olive-
green) precipitate.
35.
Ketone bodies
Normal totalketone bodies: < 1 mg/dL (0.1
mmol/L)
Ketoacidosis: > 3 mmol/L
Positive ketone bodies in urine = abnormal
(seen in diabetes mellitus, starvation,
vomiting, etc.).
37.
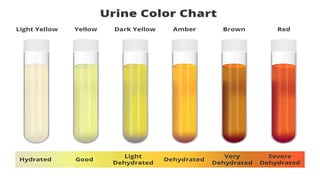
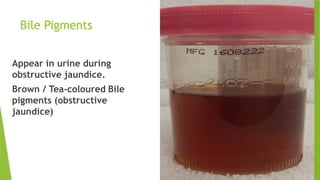
Bile Pigments
Appear inurine during
obstructive jaundice.
Brown / Tea-coloured Bile
pigments (obstructive
jaundice)
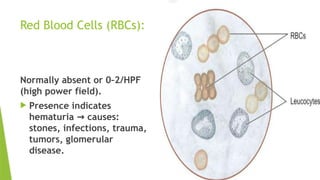
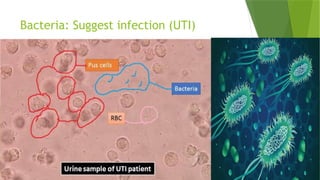
Red Blood Cells(RBCs):
Normally absent or 0–2/HPF
(high power field).
Presence indicates
hematuria causes:
→
stones, infections, trauma,
tumors, glomerular
disease.
41.
White Blood Cells(WBCs):
Normally absent or
0–5/HPF.
Increased in urinary tract
infections (UTI),
pyelonephritis, cystitis.
42.
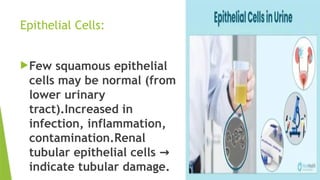
Epithelial Cells:
Few squamousepithelial
cells may be normal (from
lower urinary
tract).Increased in
infection, inflammation,
contamination.Renal
tubular epithelial cells →
indicate tubular damage.
43.
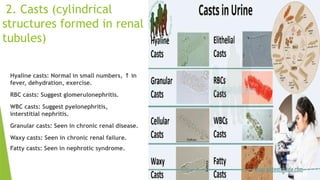
2. Casts (cylindrical
structuresformed in renal
tubules)
Hyaline casts: Normal in small numbers, in
↑
fever, dehydration, exercise.
RBC casts: Suggest glomerulonephritis.
WBC casts: Suggest pyelonephritis,
interstitial nephritis.
Granular casts: Seen in chronic renal disease.
Waxy casts: Seen in chronic renal failure.
Fatty casts: Seen in nephrotic syndrome.
45.
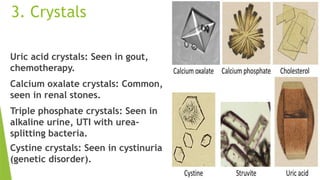
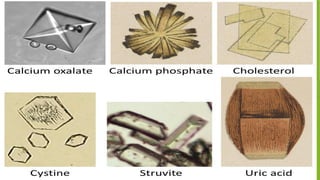
3. Crystals
Uric acidcrystals: Seen in gout,
chemotherapy.
Calcium oxalate crystals: Common,
seen in renal stones.
Triple phosphate crystals: Seen in
alkaline urine, UTI with urea-
splitting bacteria.
Cystine crystals: Seen in cystinuria
(genetic disorder).
47.
🔹 4. Microorganisms
Bacteria:Suggest infection (UTI).
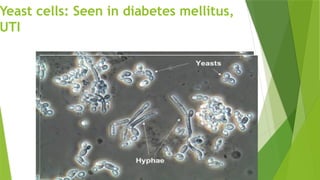
Yeast cells: Seen in diabetes
mellitus.Yeast cells in urine, known as
candiduria, can indicate a urinary tract
infection (UTI)
Parasites: Trichomonas vaginalis may be
detected.
6. Calcium &Phosphorus
Calcium: 8.5–10.5 mg/dL
Phosphorus: 2.5–4.5 mg/dL
Imbalance common in chronic kidney
disease (CKD) due to altered Vitamin D
metabolism.
60.
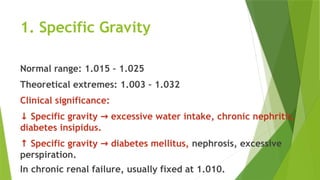
7. Glomerular FiltrationRate (GFR)
Estimated from Serum Creatinine using
formulas.
Normal GFR: 90–120 mL/min/1.73m²
<60 Chronic kidney disease (if
→
persistent).