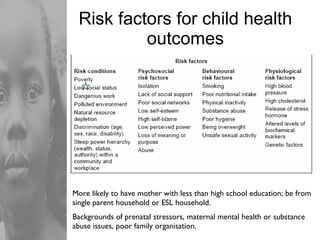
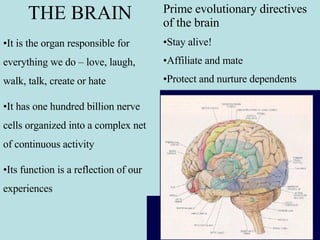
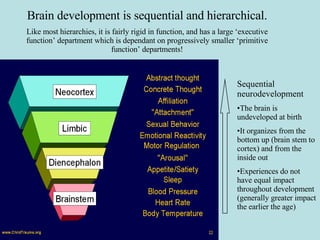
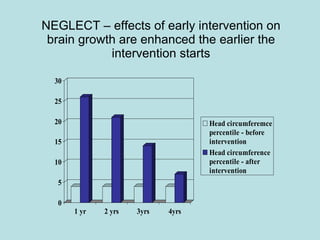
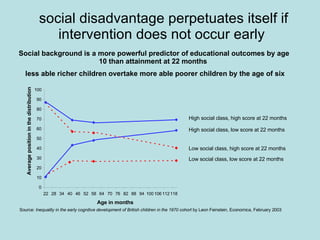
The document discusses the importance of early childhood development and the impacts of trauma on children. It notes that early experiences shape lifelong patterns of behavior by changing the brain's structure and function. Childhood trauma, neglect, and poor attachment can negatively impact cognitive, emotional, social, and behavioral development, with effects often persisting into adulthood. Research on child development has led to understanding how to advantage children through supportive early experiences.