
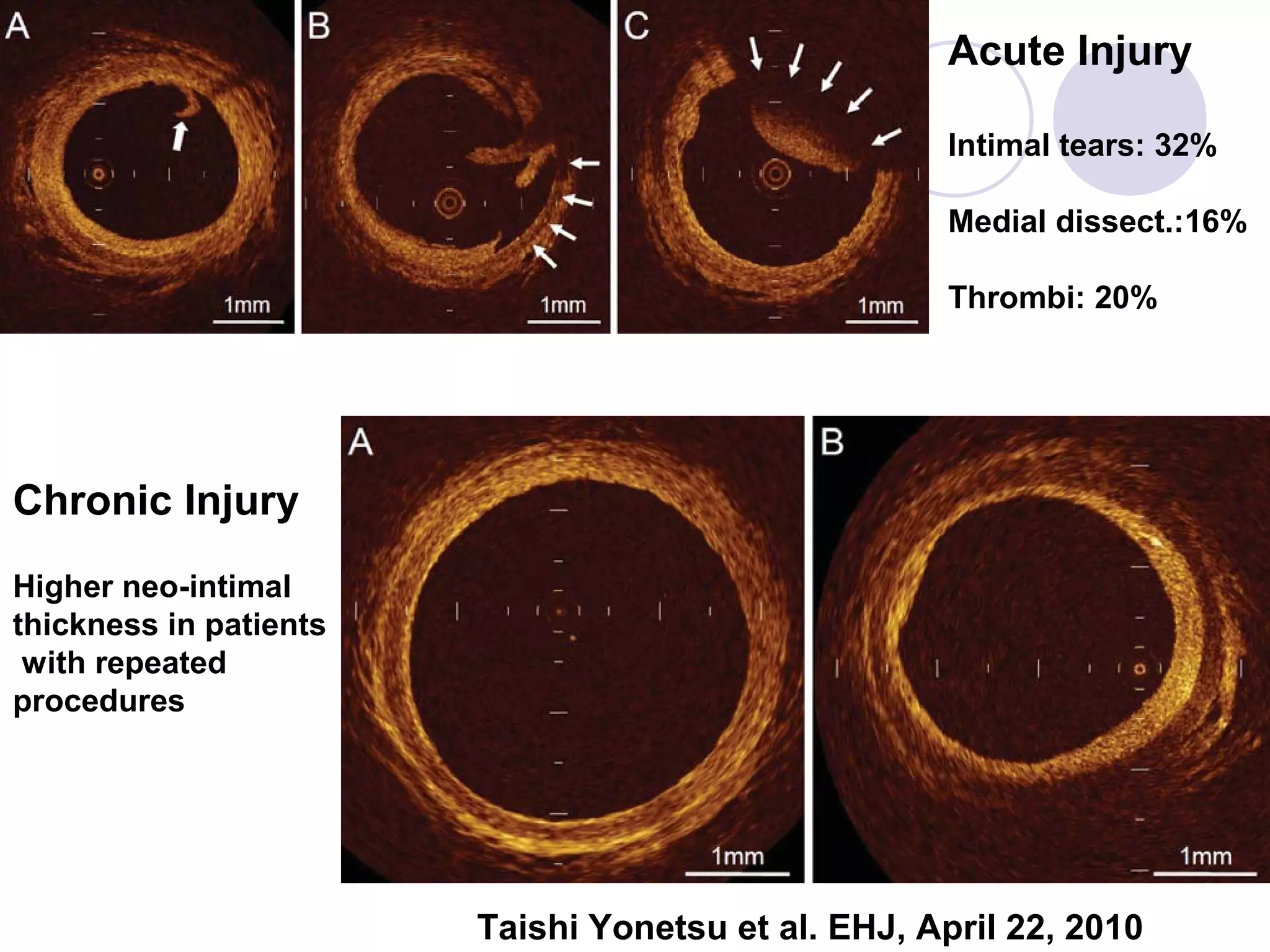
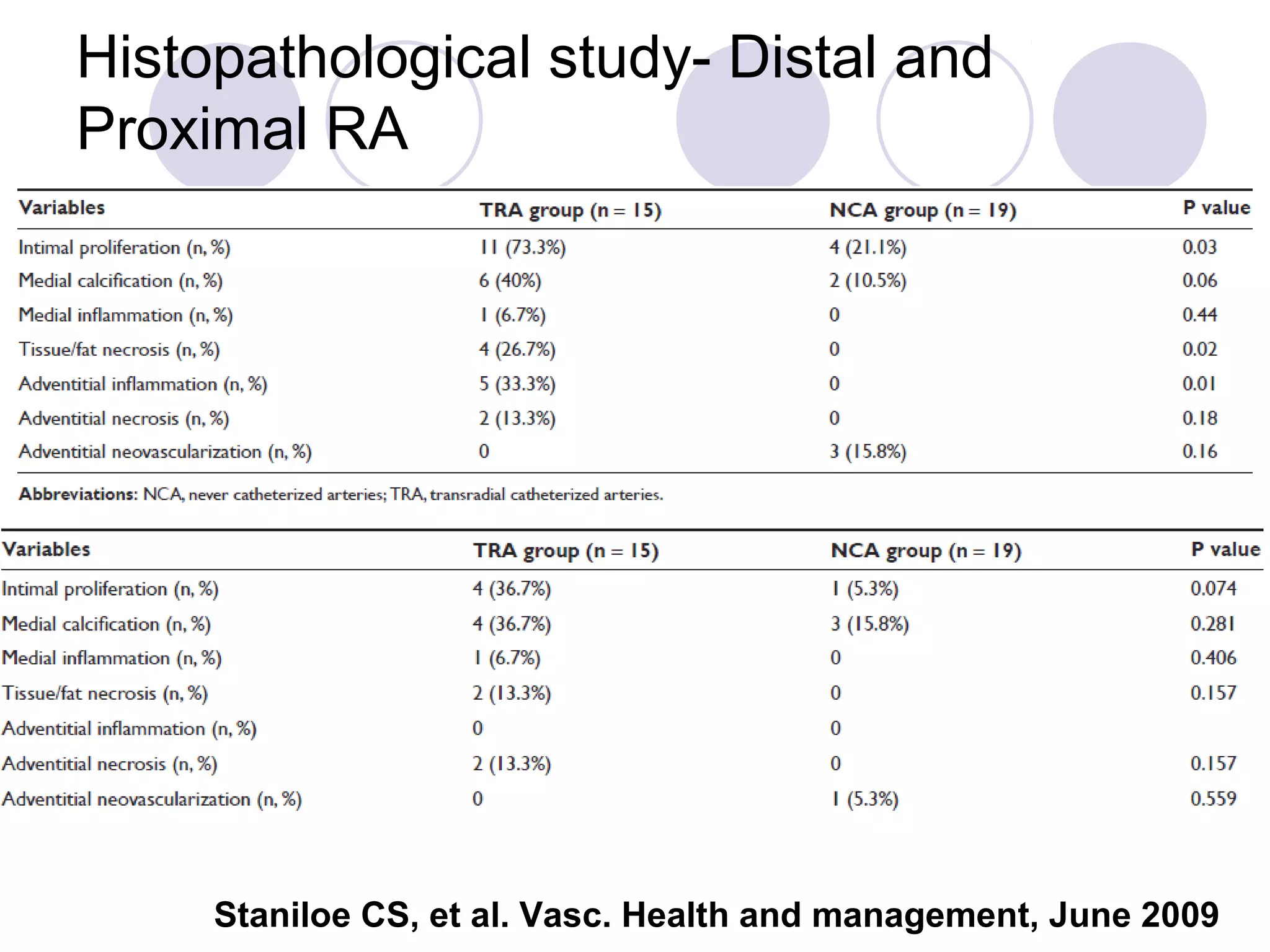
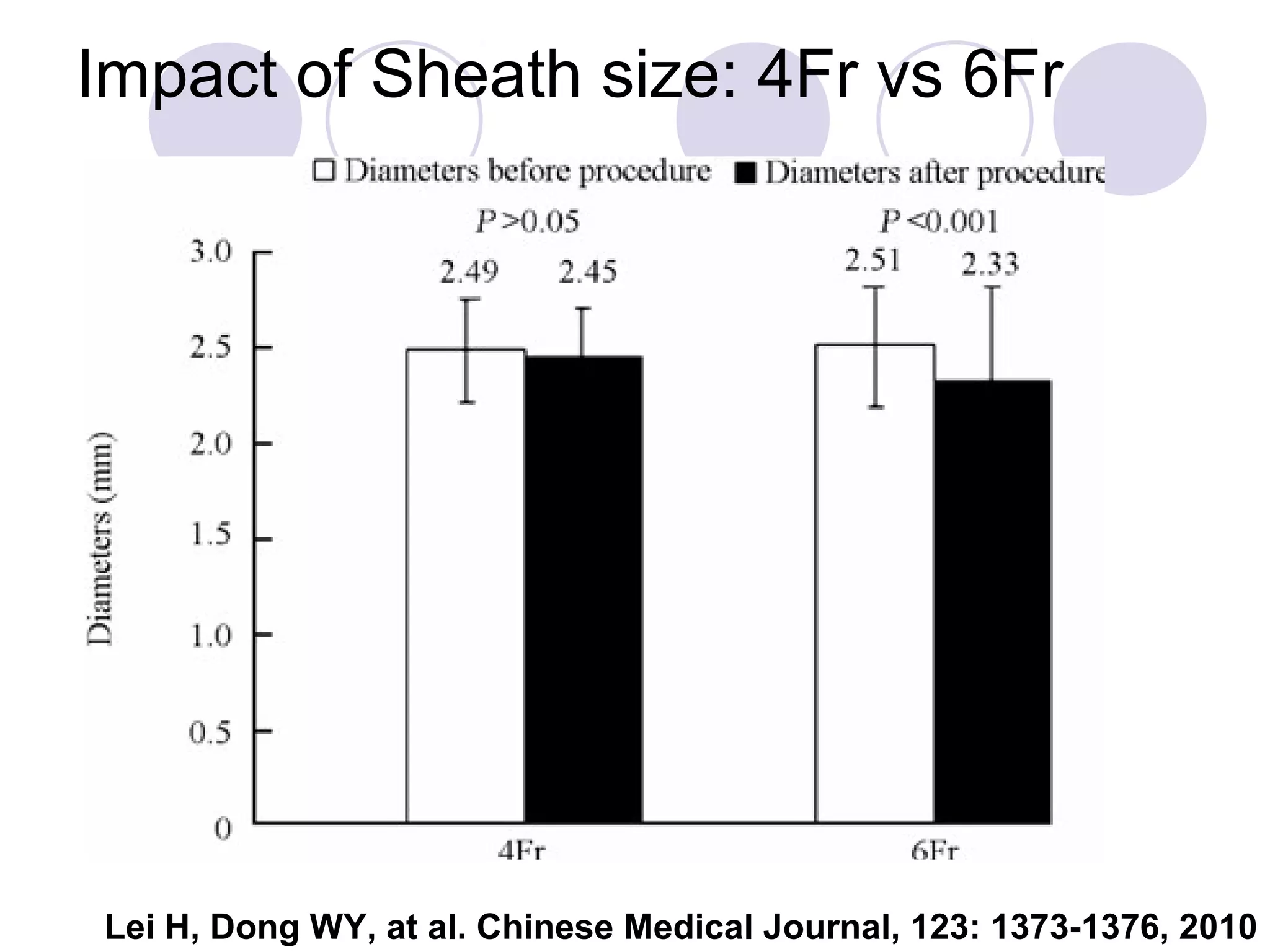
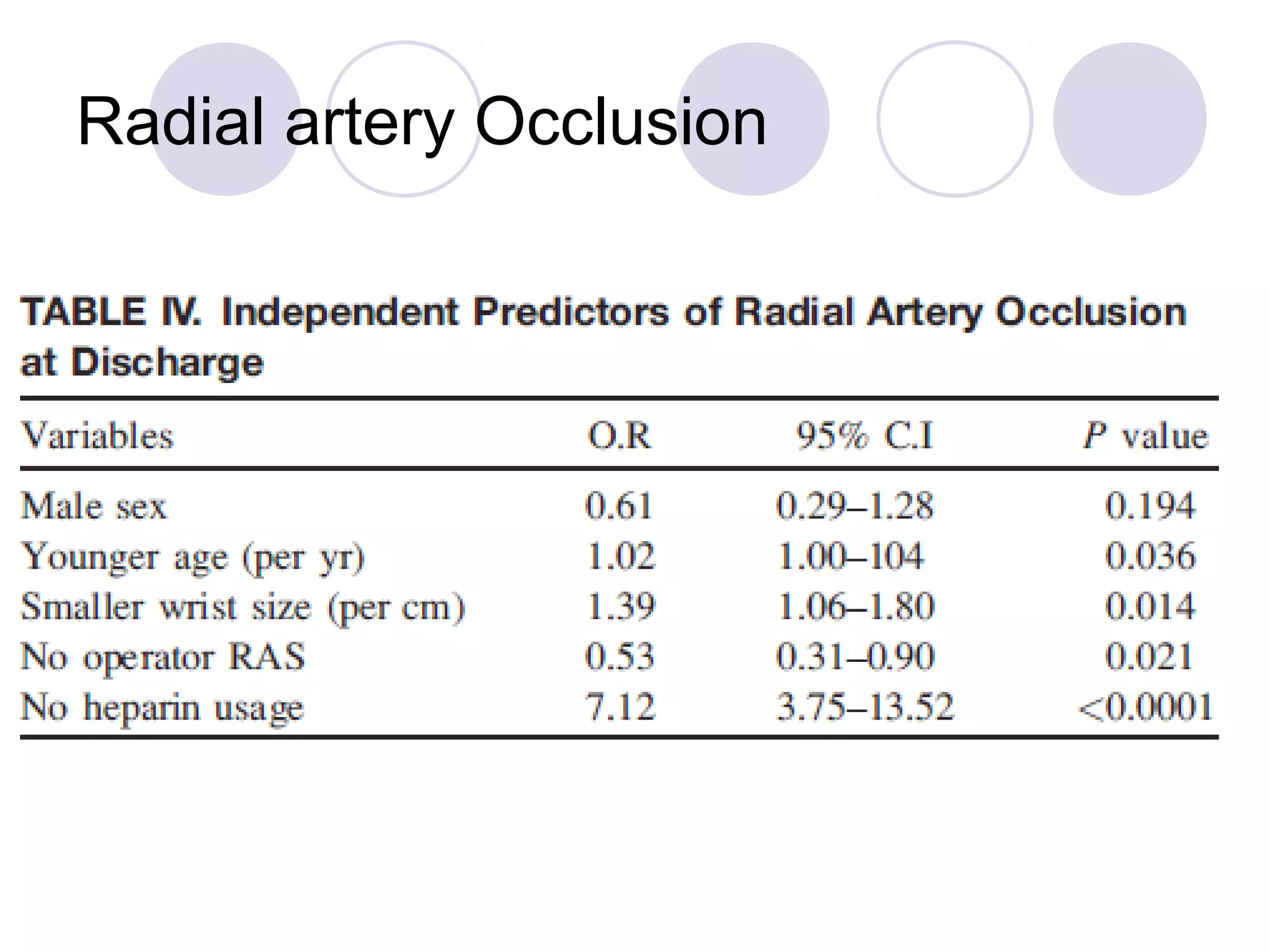
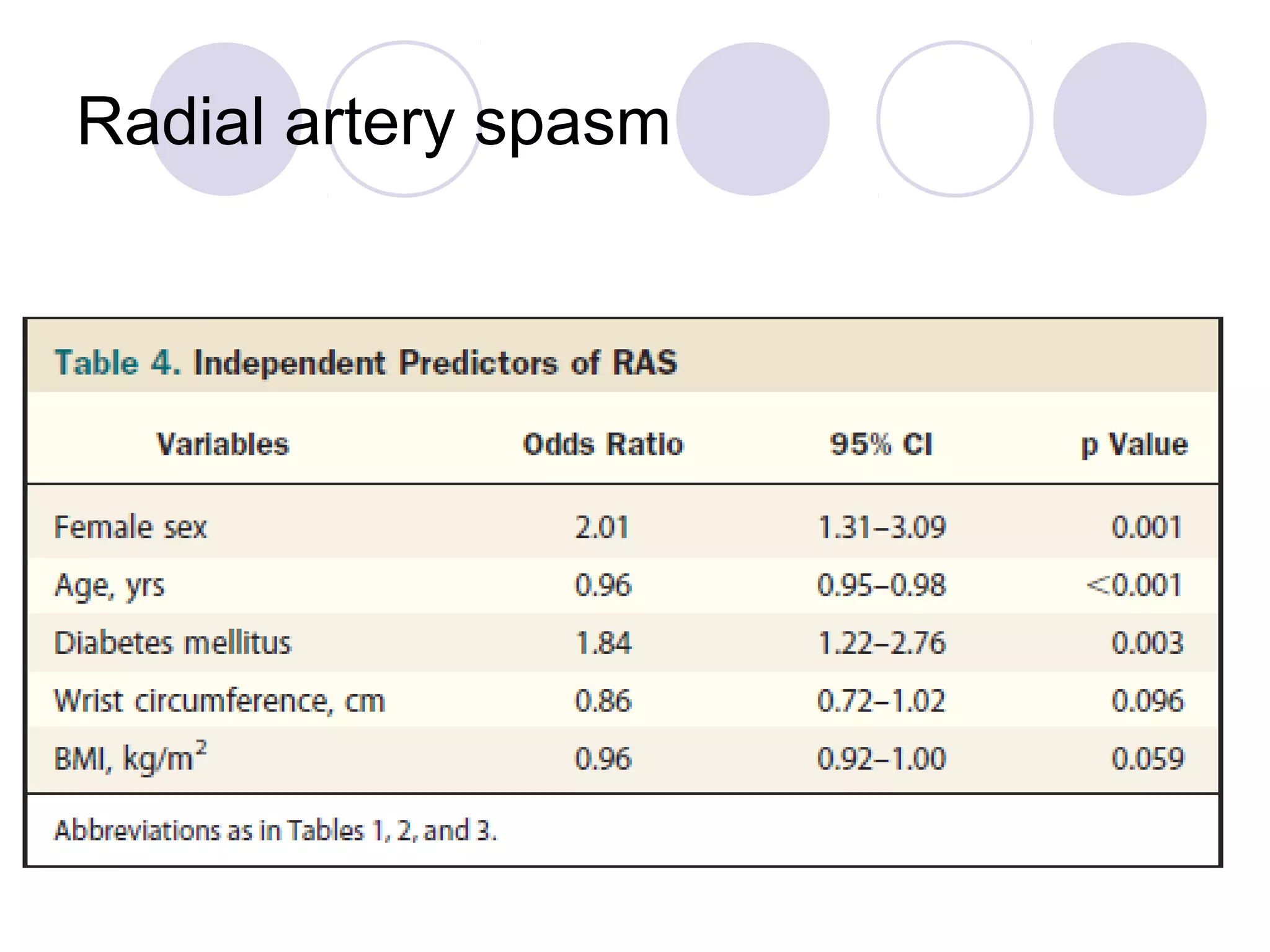
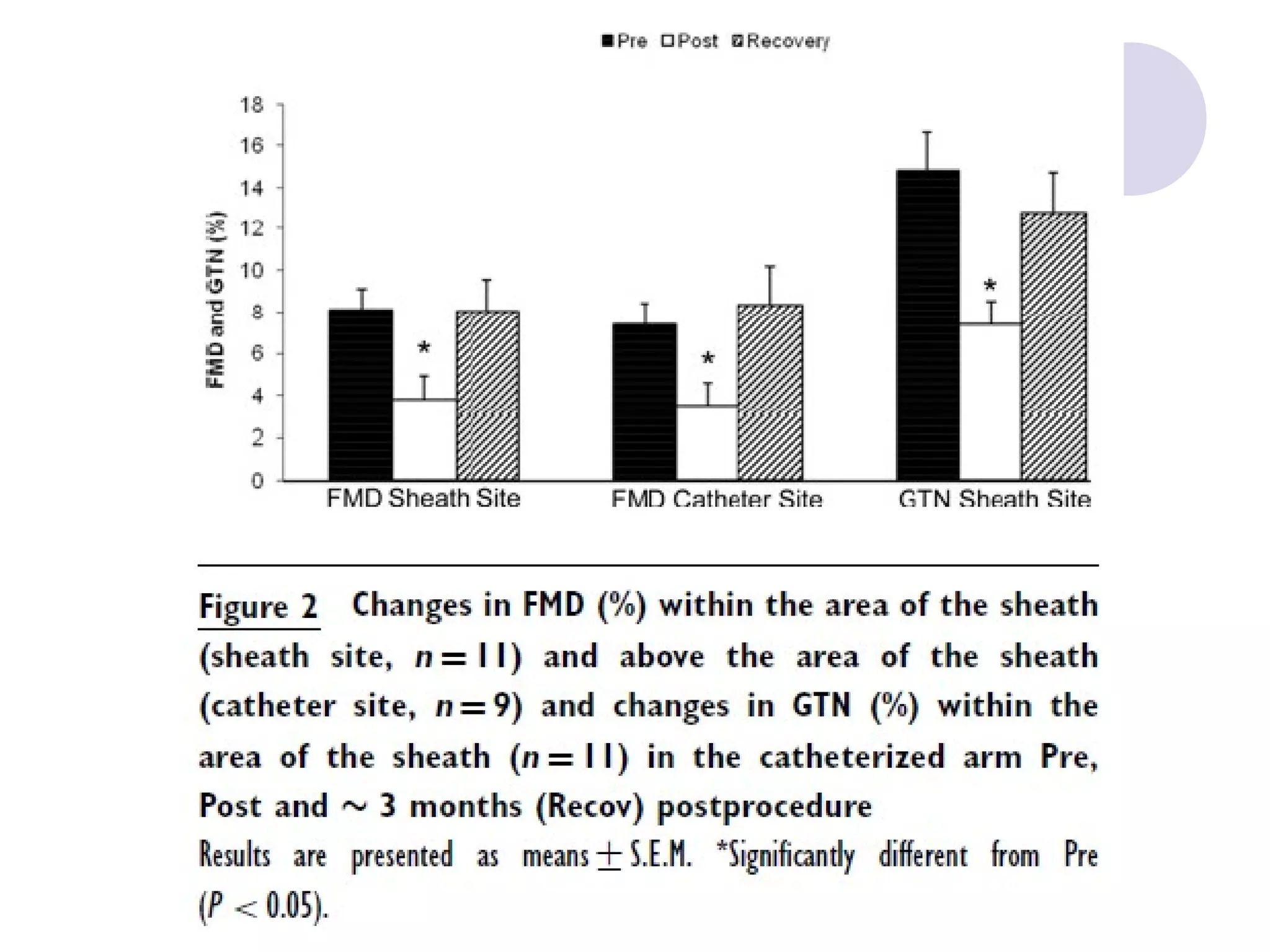
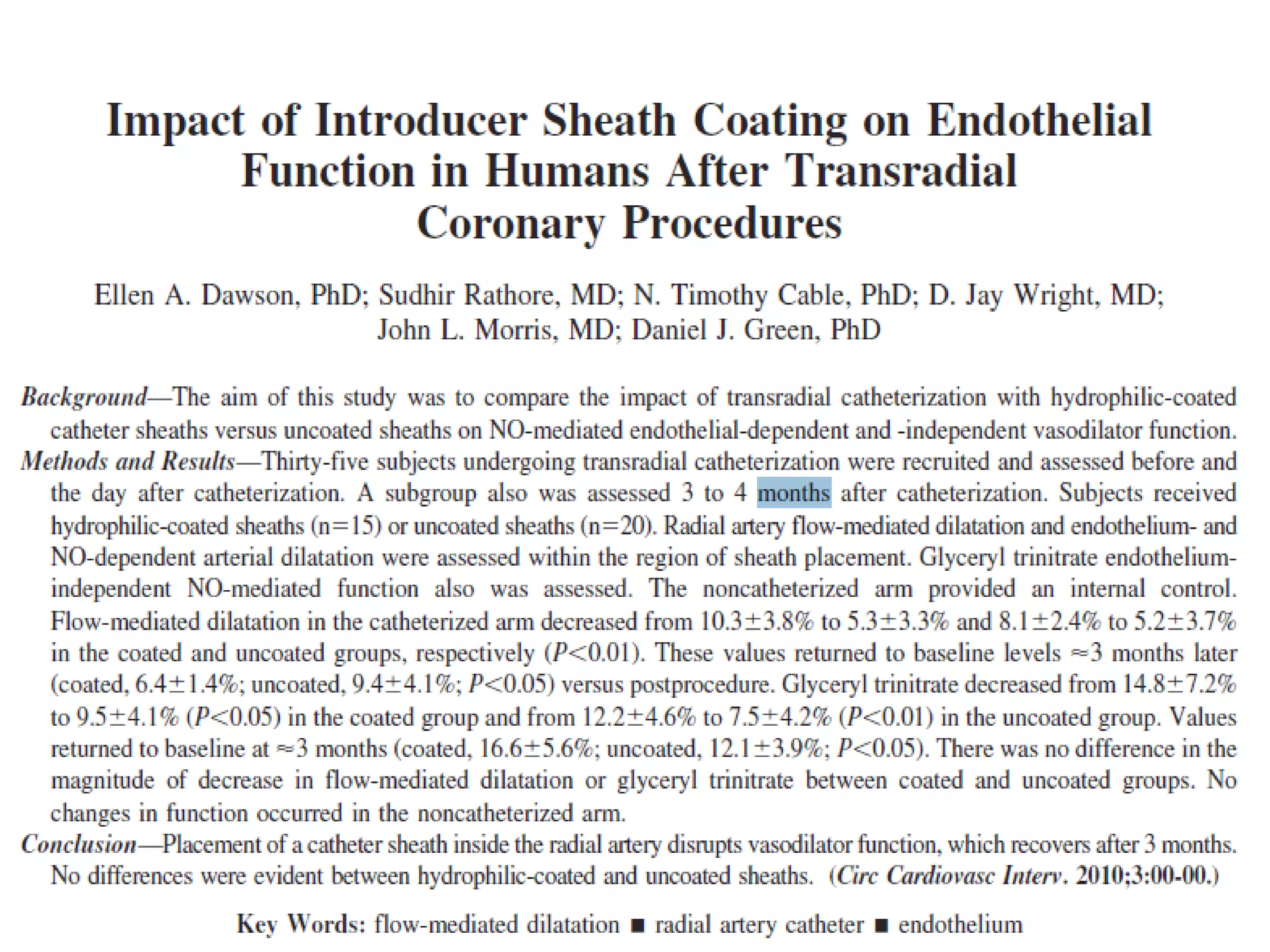
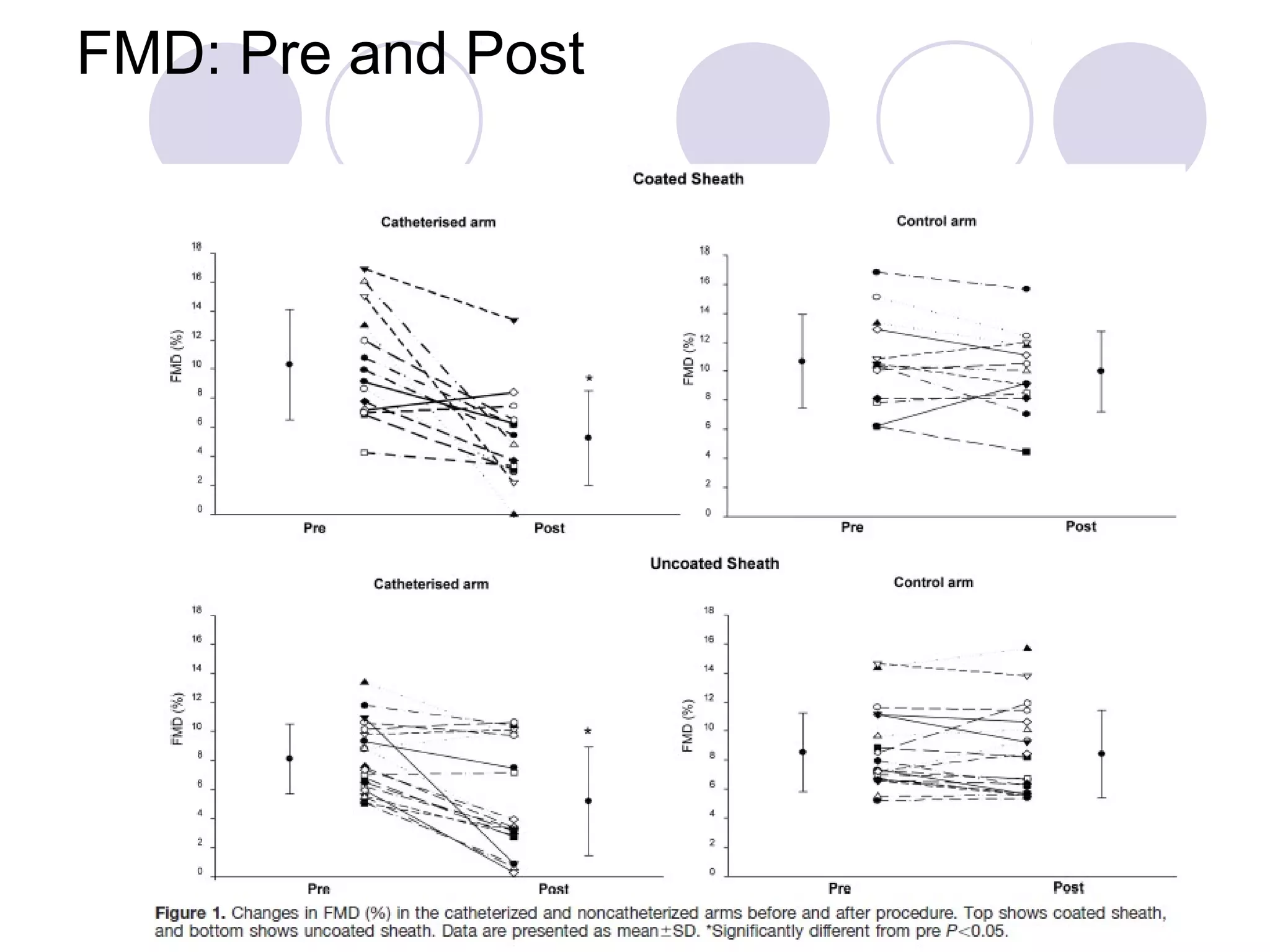
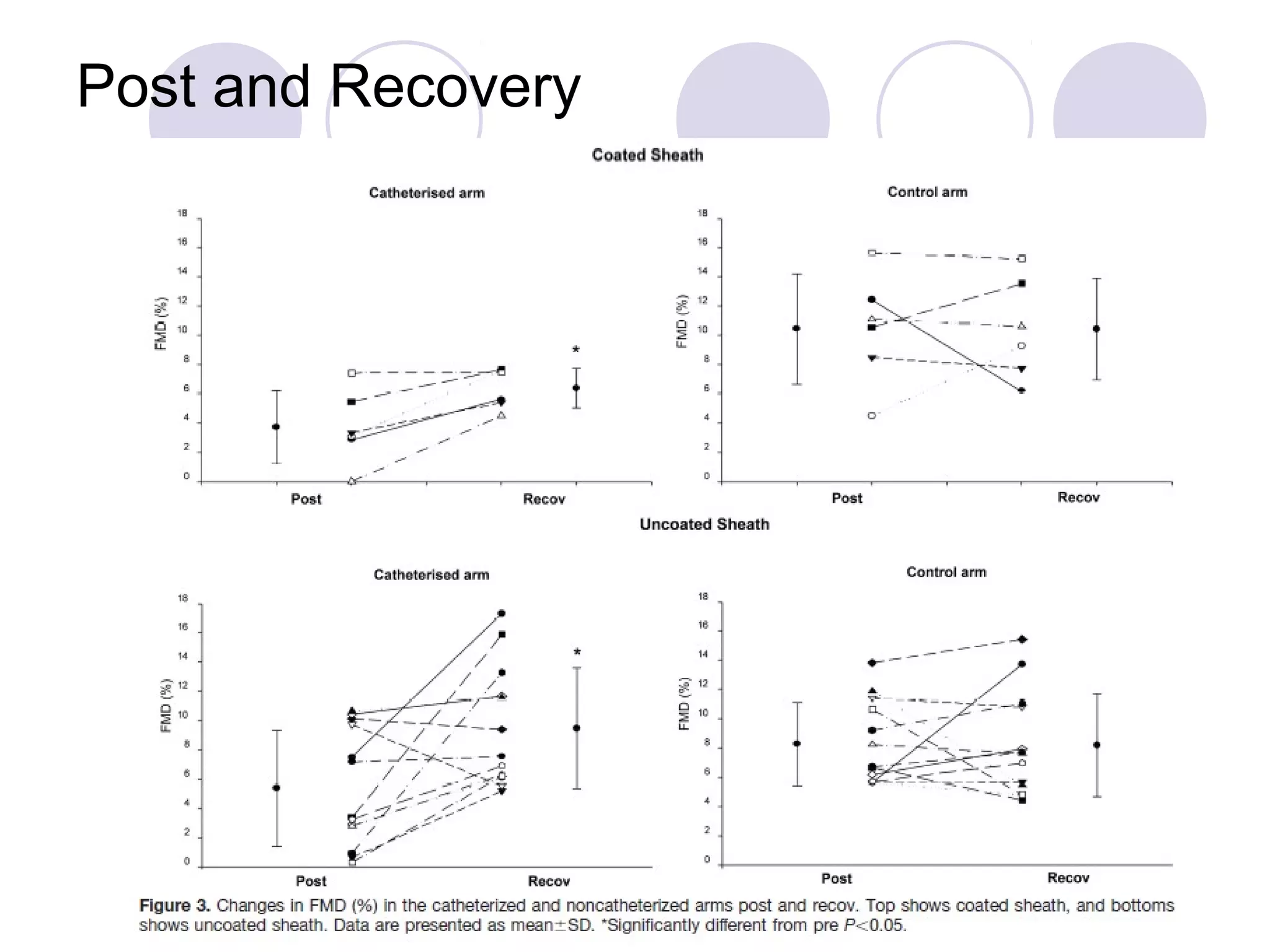
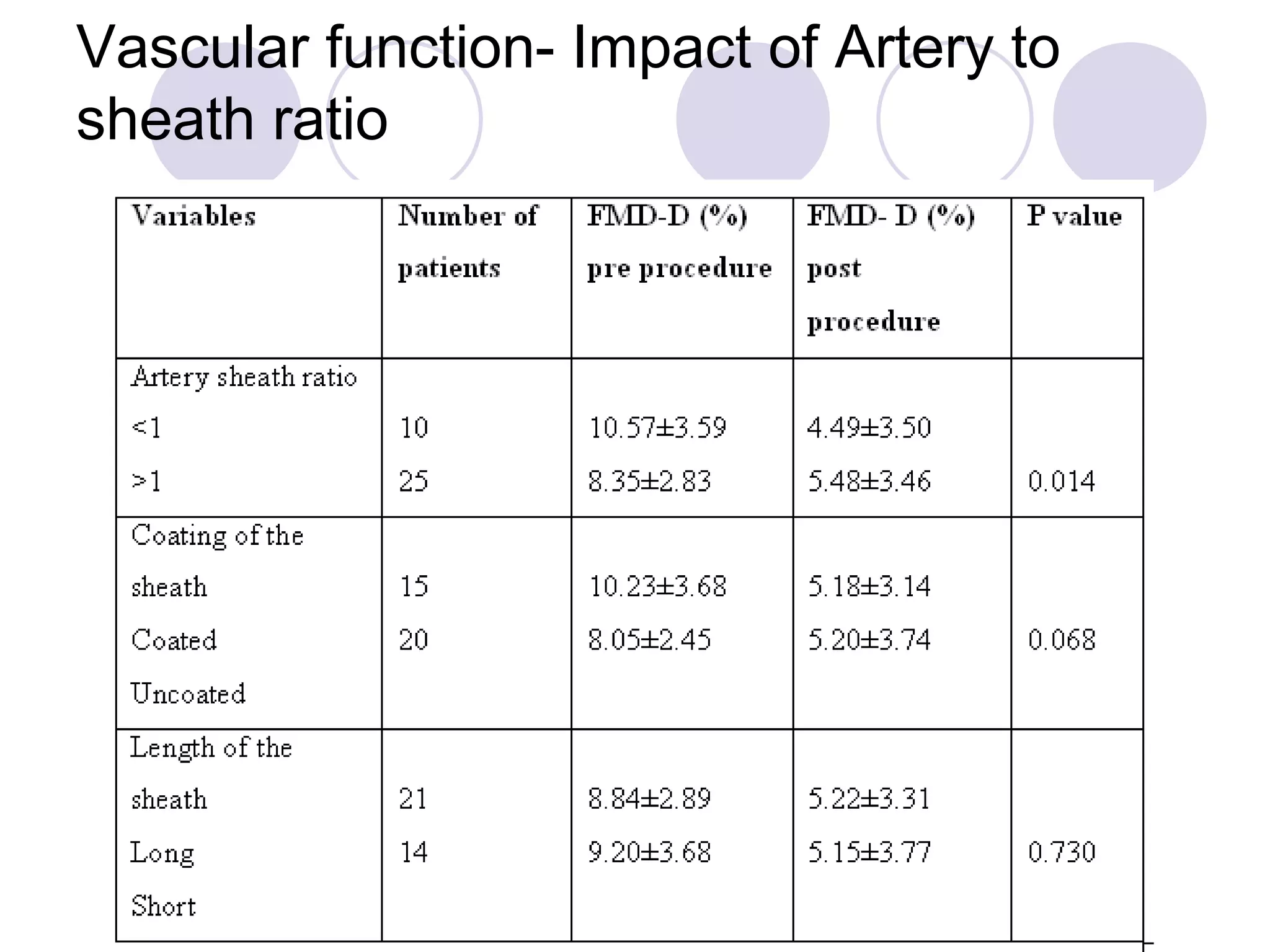
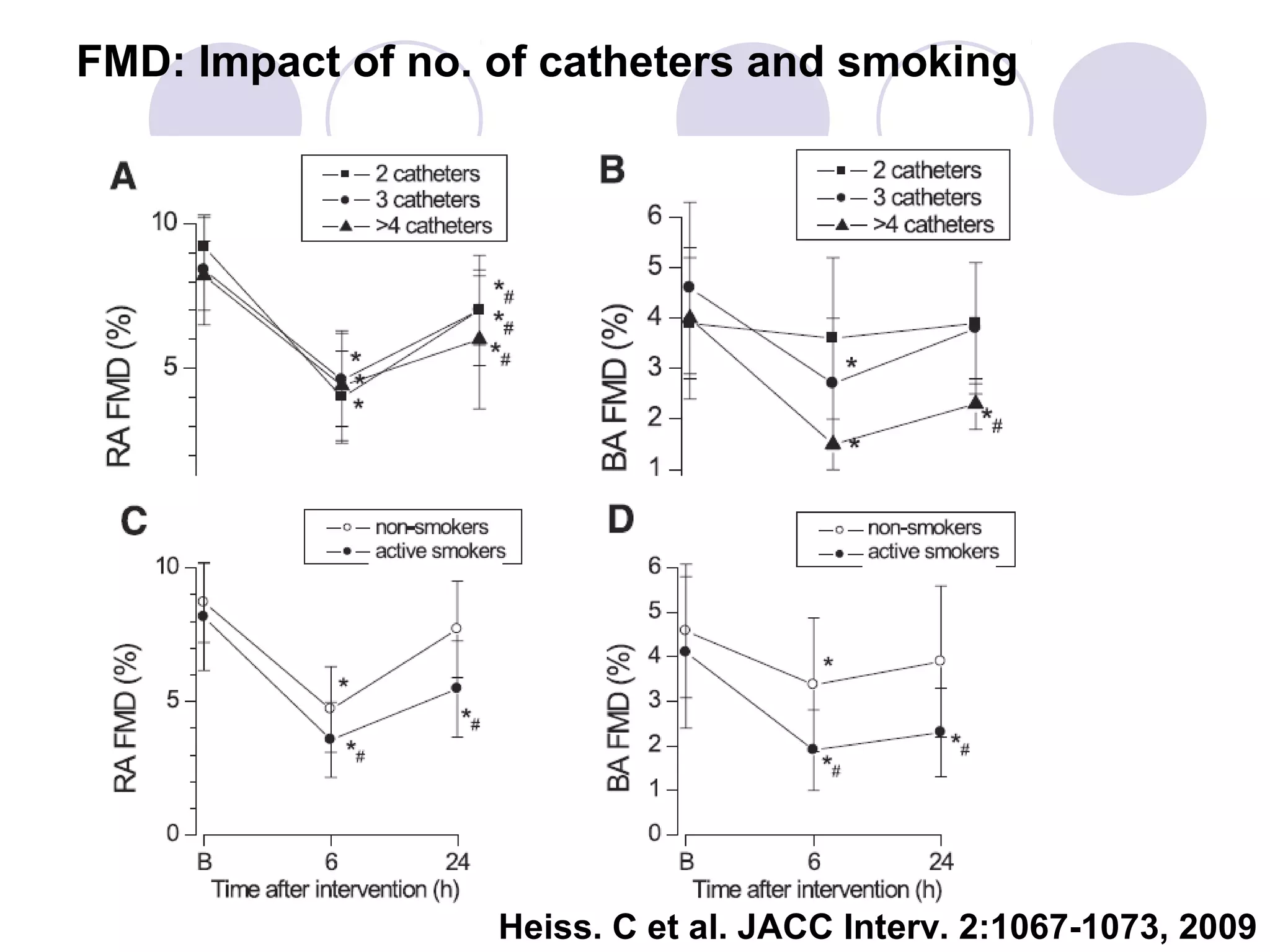
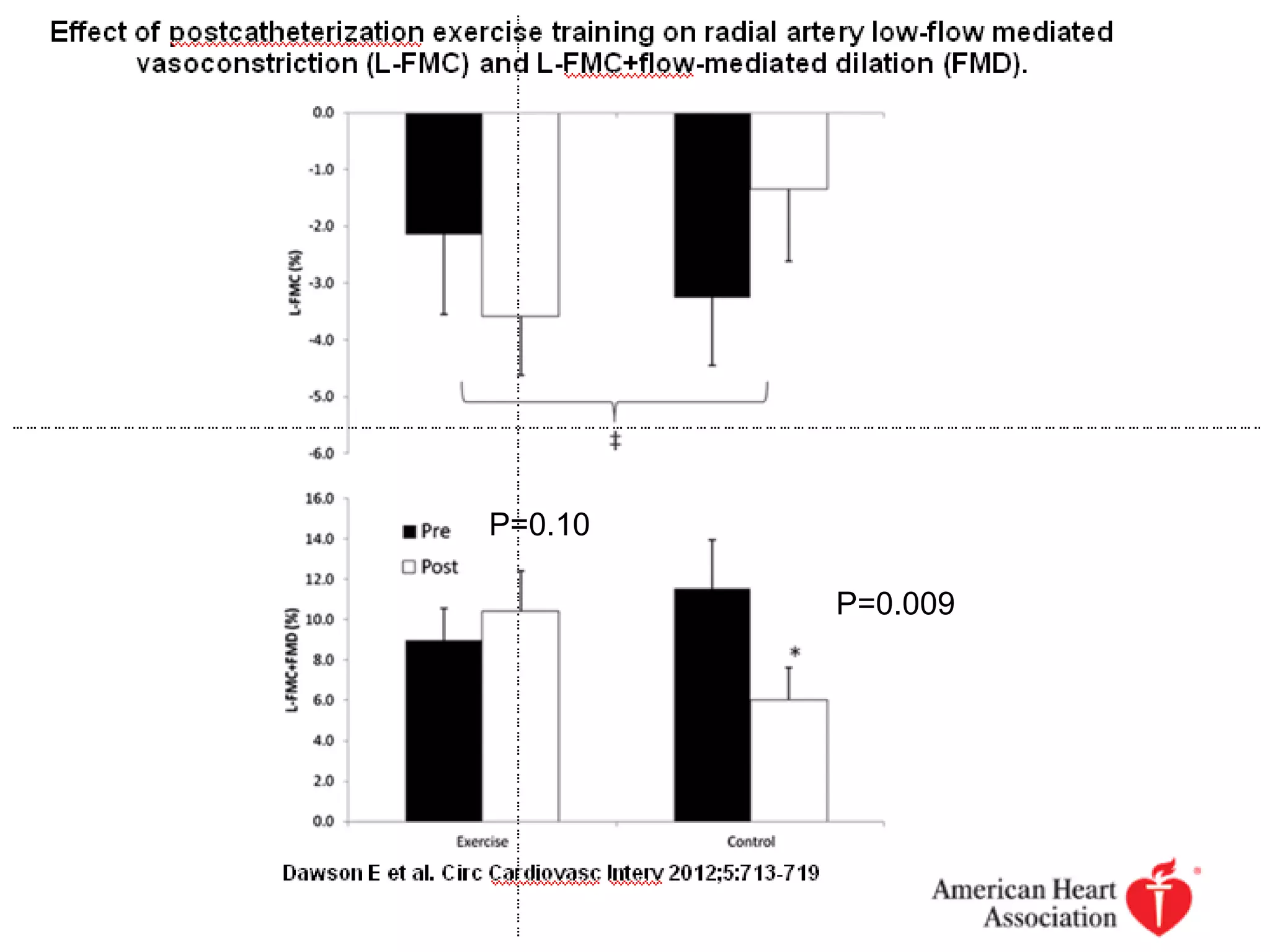
This document summarizes research on non-occlusive radial artery injury from transradial procedures. It discusses: 1. Historical studies found non-occlusive injuries like neointimal hyperplasia and stenosis in around 50% of patients after repeated procedures. 2. Acute injuries include intimal tears, dissections, and thrombi, while chronic injuries involve increased neointimal thickness in patients with repeat procedures. 3. Larger sheath sizes, more catheters used, lack of heparin, and patient risk factors like smoking are linked to greater radial artery injury. 4. Endothelial dysfunction occurs after procedures but recovers by 3 months; exercise training may aid recovery












































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)










