
Downloaded 11 times



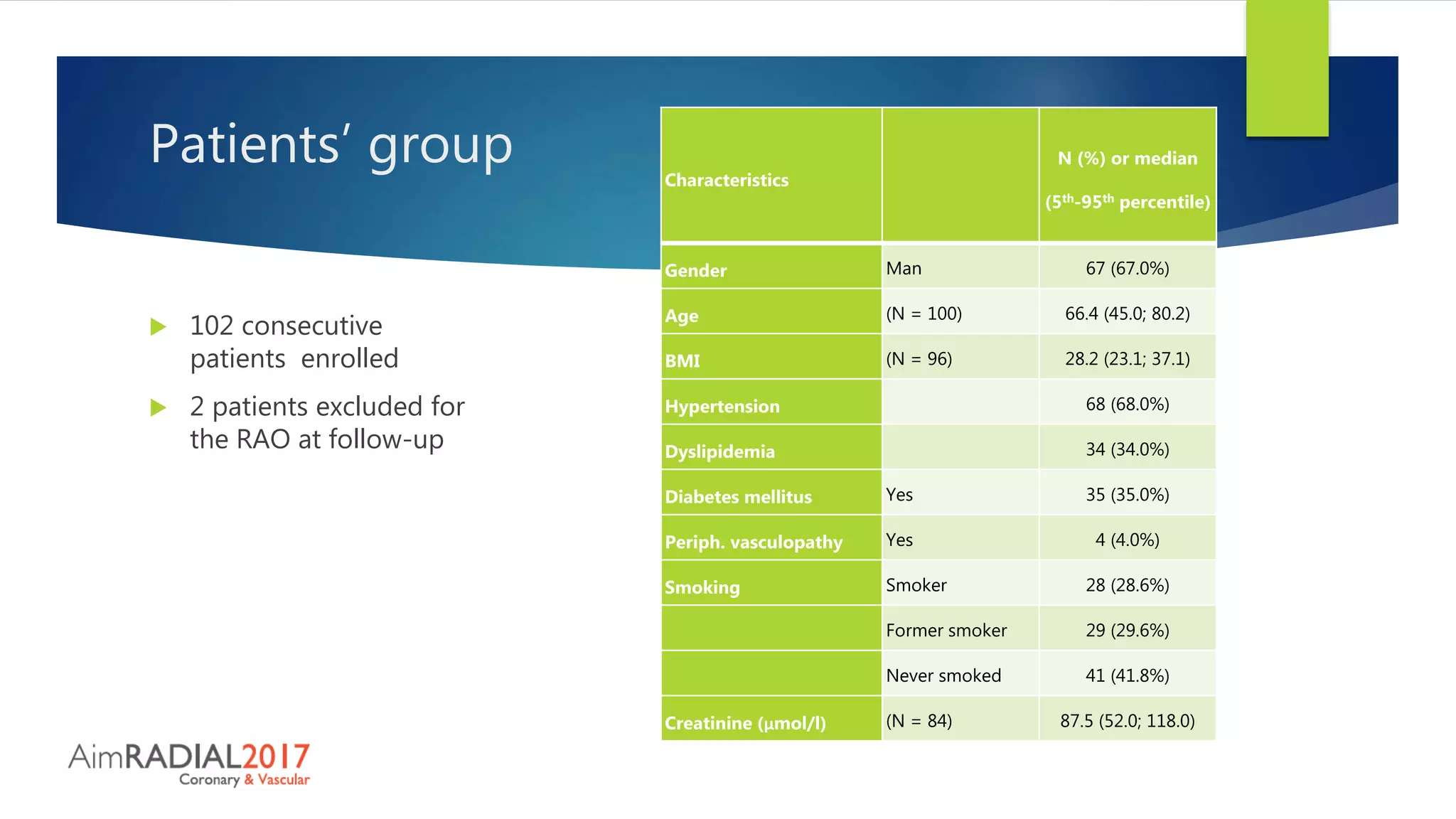
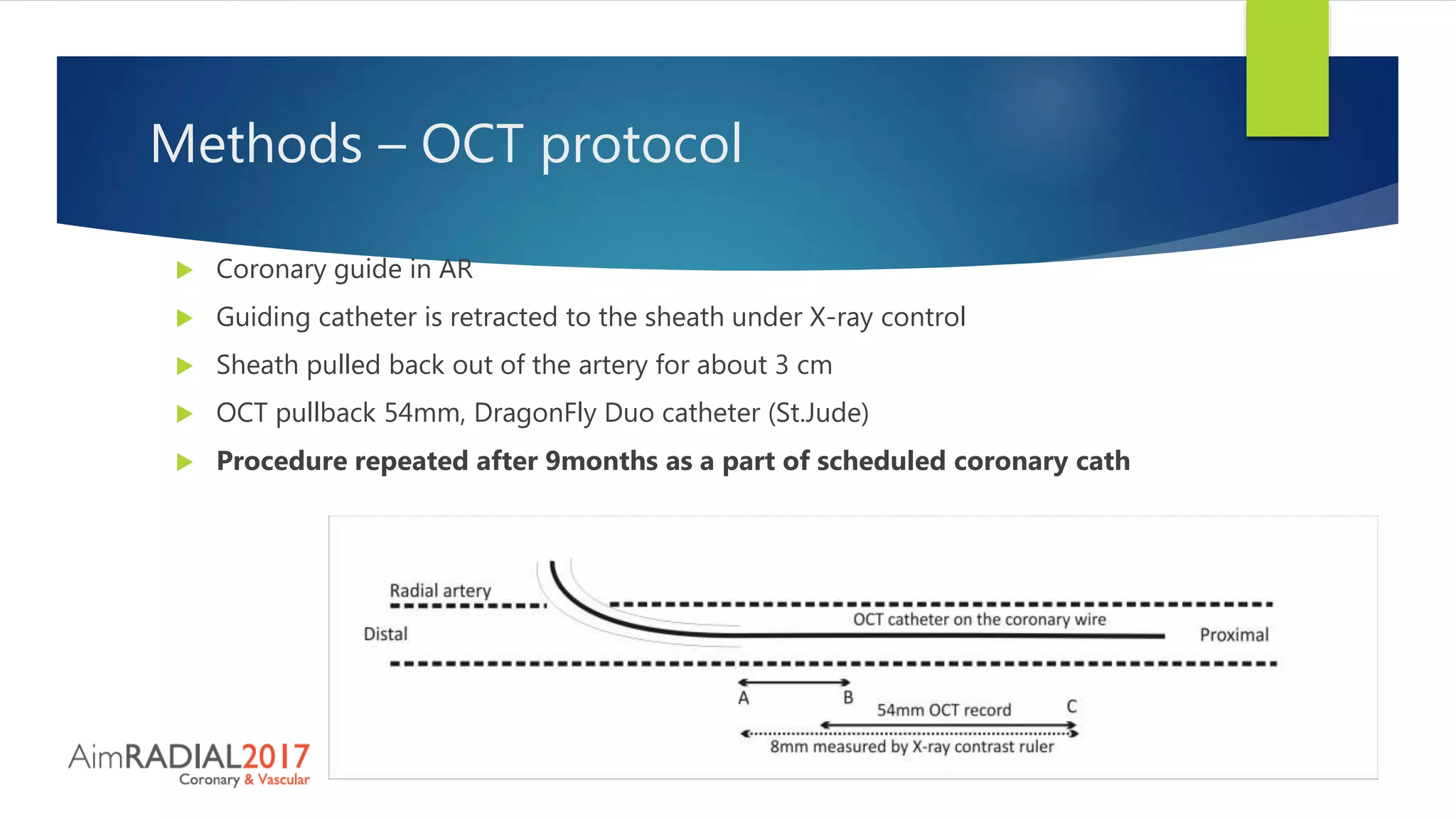


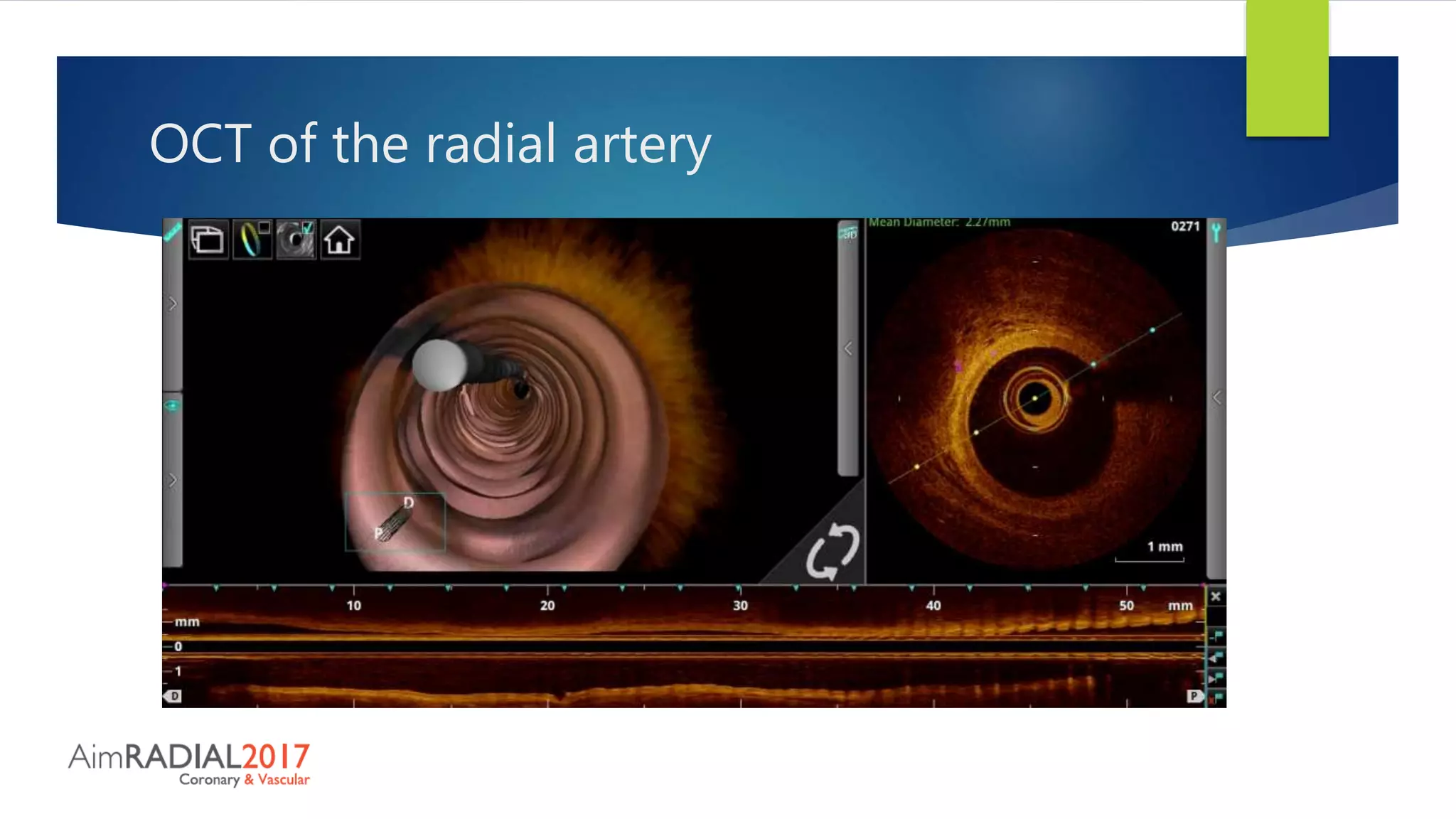
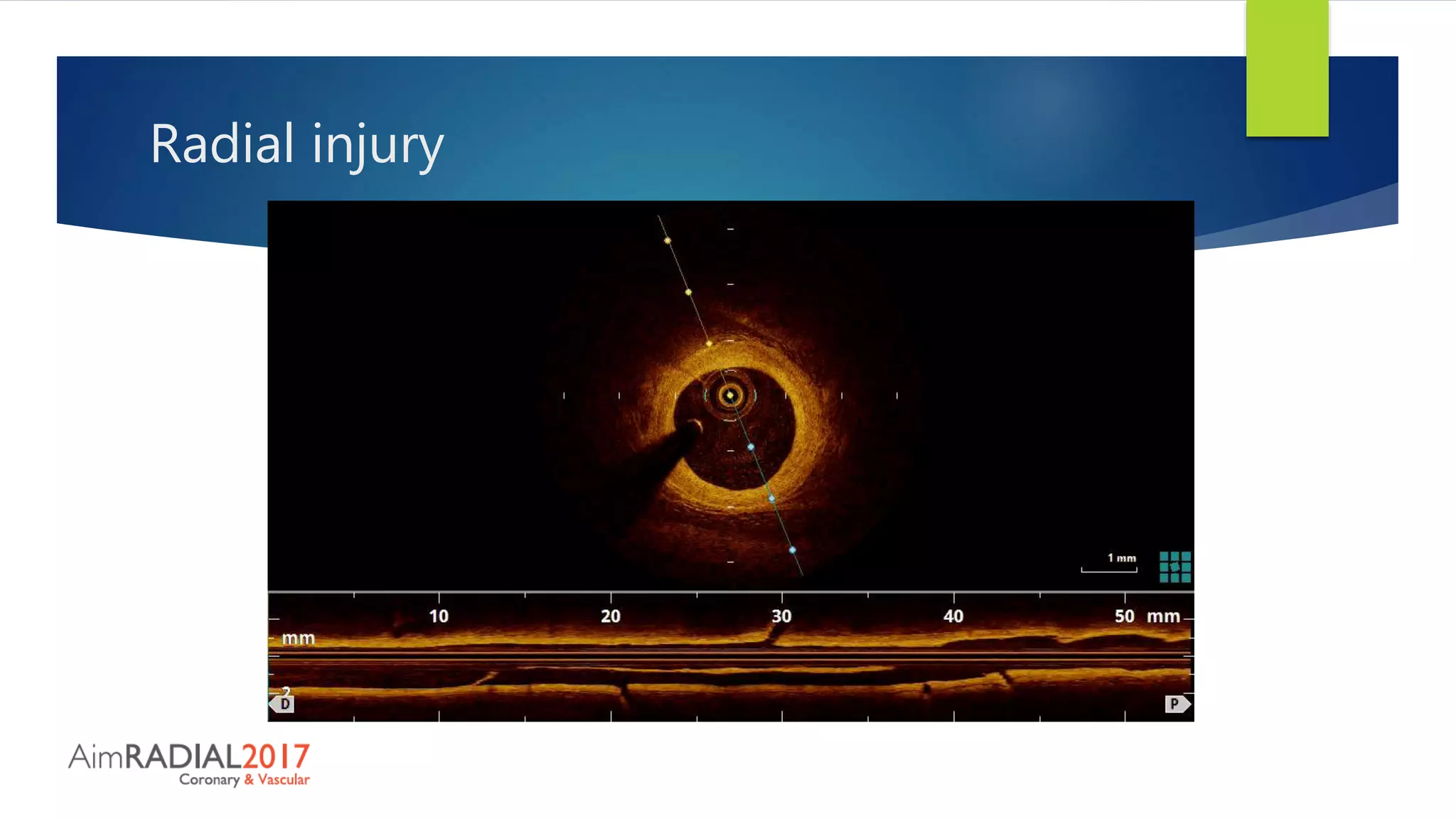
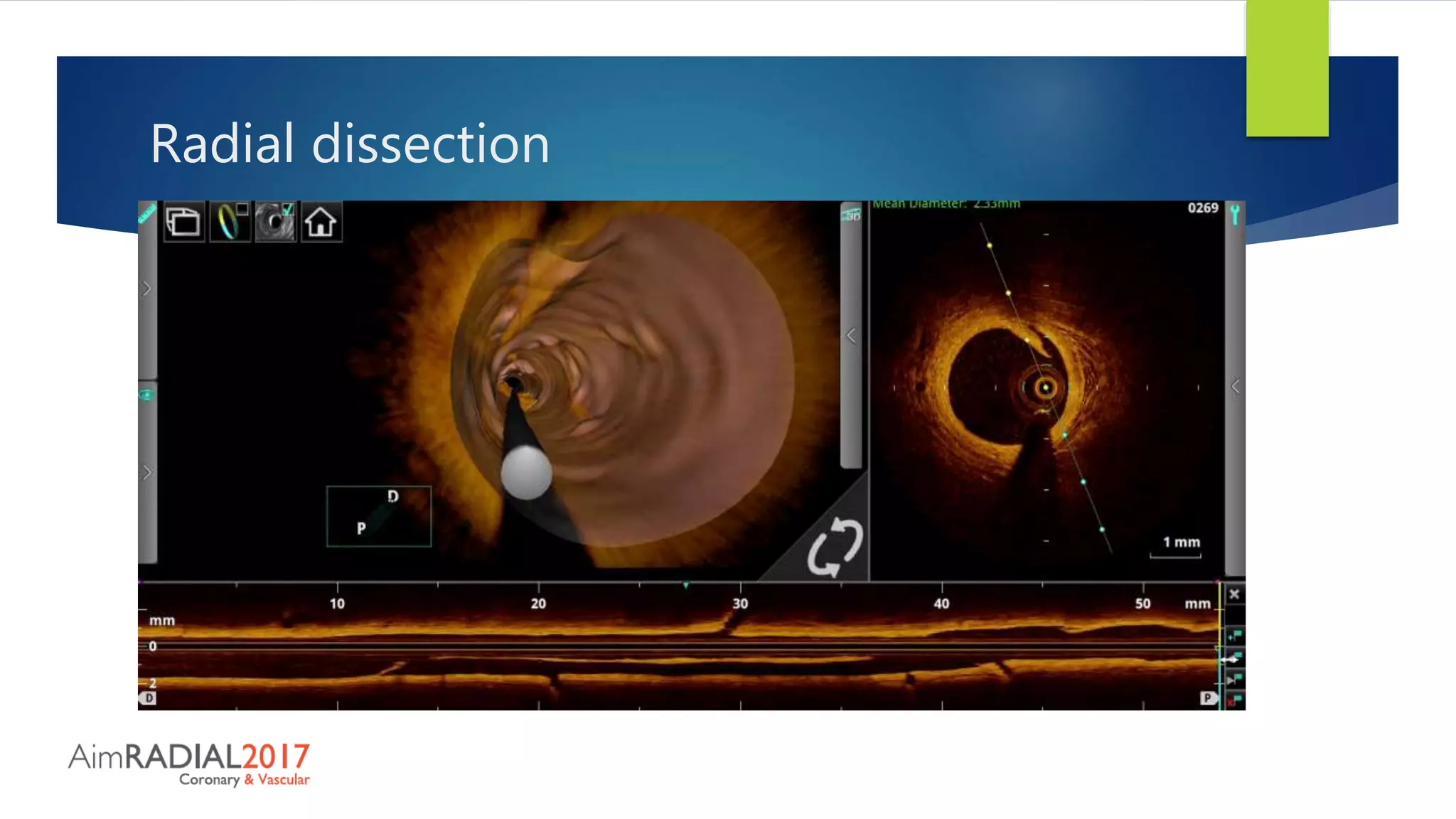



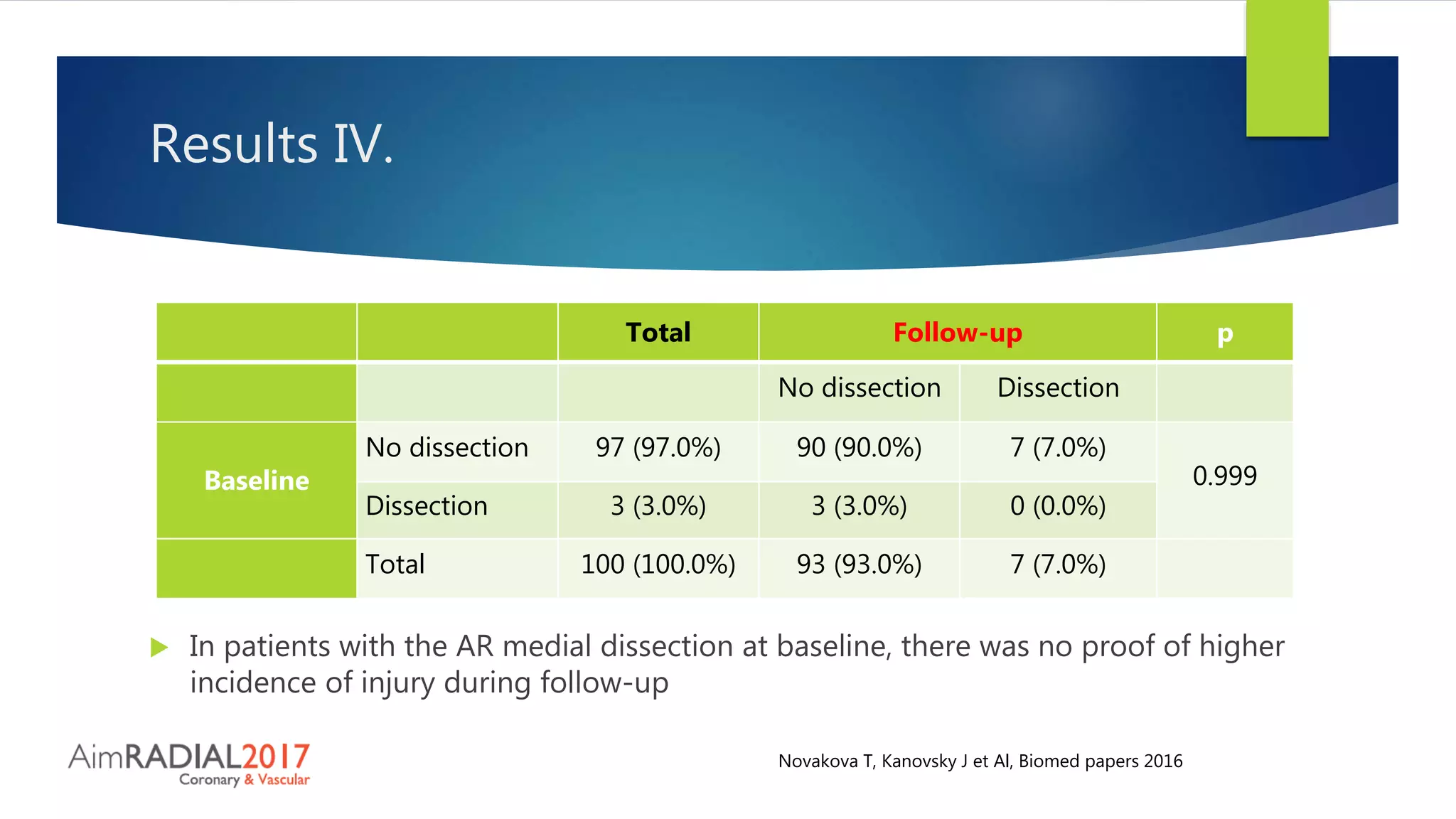



This study evaluated radial artery injury after percutaneous coronary intervention (PCI) using optical coherence tomography (OCT) at baseline and 9-month follow up in 100 patients. At baseline, 11% had intimal tears and 3% had medial dissections. At follow up, 10% had intimal tears and 7% had medial dissections, with no significant differences between time points. Compared to prior studies using longer sheaths, this study found a lower number of radial artery injuries, possibly due to the use of shorter 7cm sheaths. Serial OCT analysis found no persistent changes in arteries with initial injuries. This suggests short sheath use may reduce radial artery injury risk after transradial PCI.



































































