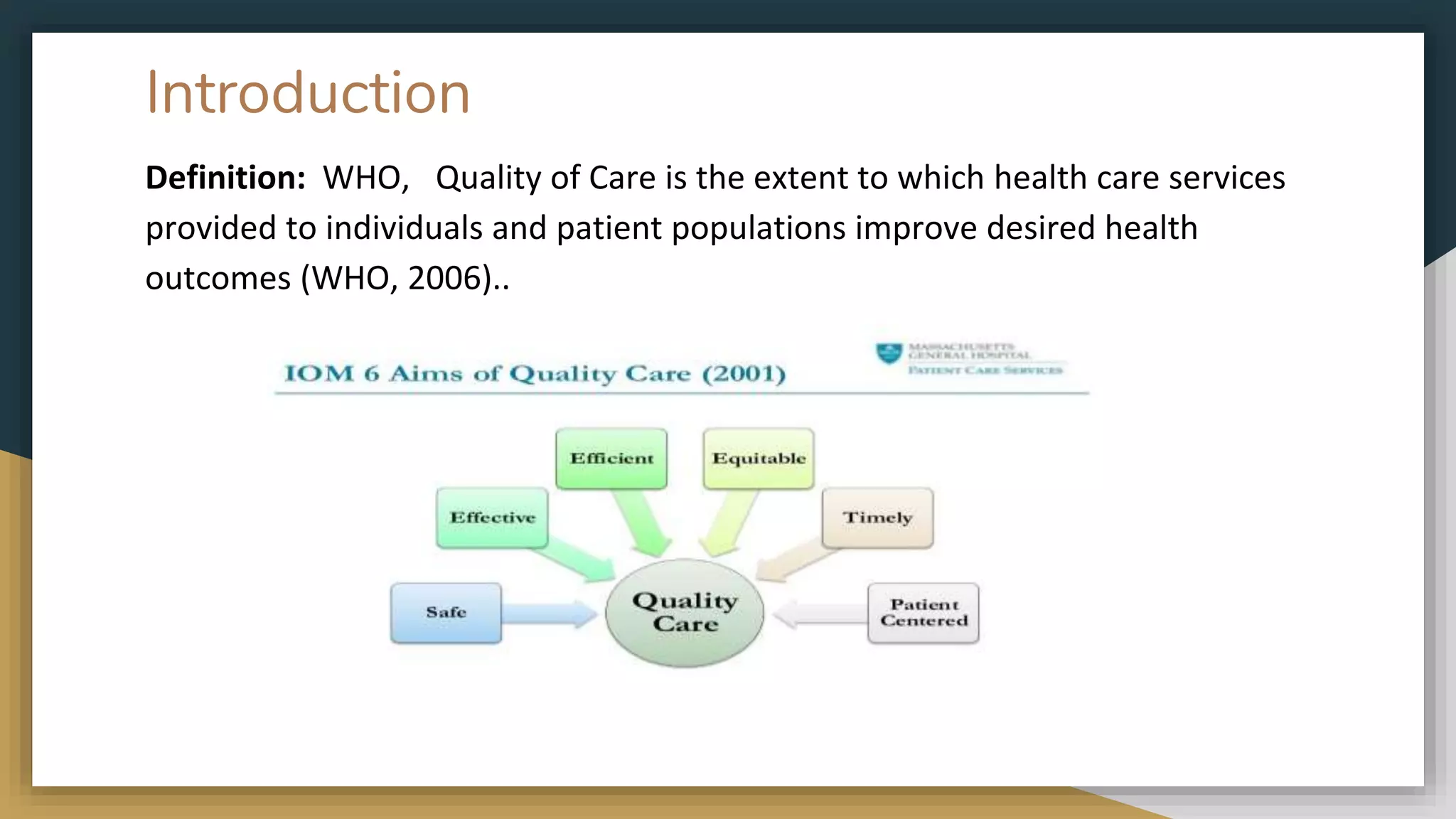
This document discusses quality of care in healthcare. It defines quality of care according to the WHO as services that improve desired health outcomes. The aims of quality care are identified as safe, effective, timely, efficient and equitable care. Key indicators of quality are also outlined, such as medication errors, bed sores, and urinary tract infections. Improving quality can provide patient-centered care and increase access. Challenges include lack of consent, disrespectful care, and discrimination. The conclusion advocates assessing risks, reporting incidents, engaging in prevention, and providing education to enhance quality of care.