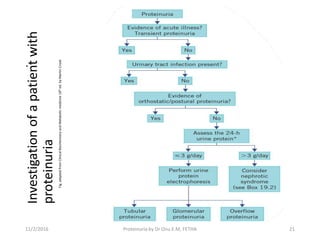
The document provides an in-depth clinical presentation on proteinuria, defining it as excessive protein in urine, with normal levels being less than 150 mg/24 hours. It discusses types of proteinuria, testing methods, limitations of screening tests, and treatment options, emphasizing the importance of identifying underlying causes and potential referrals to a nephrologist. Key classifications include glomerular and tubular proteinuria, with respective diagnostic features and management strategies outlined.


















![[2015] hepatic encephalopathy](https://cdn.slidesharecdn.com/ss_thumbnails/2015hepaticencephalopathy-151117004212-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)






























![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)

















