Downloaded 56 times




![* This theory depends on some assumptions are as follows:-
i) The GIT is simple lipoidal barrier for transport of drug.
ii) Larger the fraction of unionized drug, faster the absorption
ii) Greater the lipophilicity of unionized drug, better the absorption.
a) Pka of drug:-
Amount of drug that exist in unionized form and in ionized form is a function of
pKa of drug & pH of the fluid at the absorption site and it can be determined by
Henderson-hesselbach equation:
* pH = pKa + log [lionized form/ unionised form ]……….For, weakly acidic
drugs](https://image.slidesharecdn.com/transportmodelfinal-220618160641-bb635fac/75/Properties-of-GI-tract-pH-partition-hypothesis-9-2048.jpg)









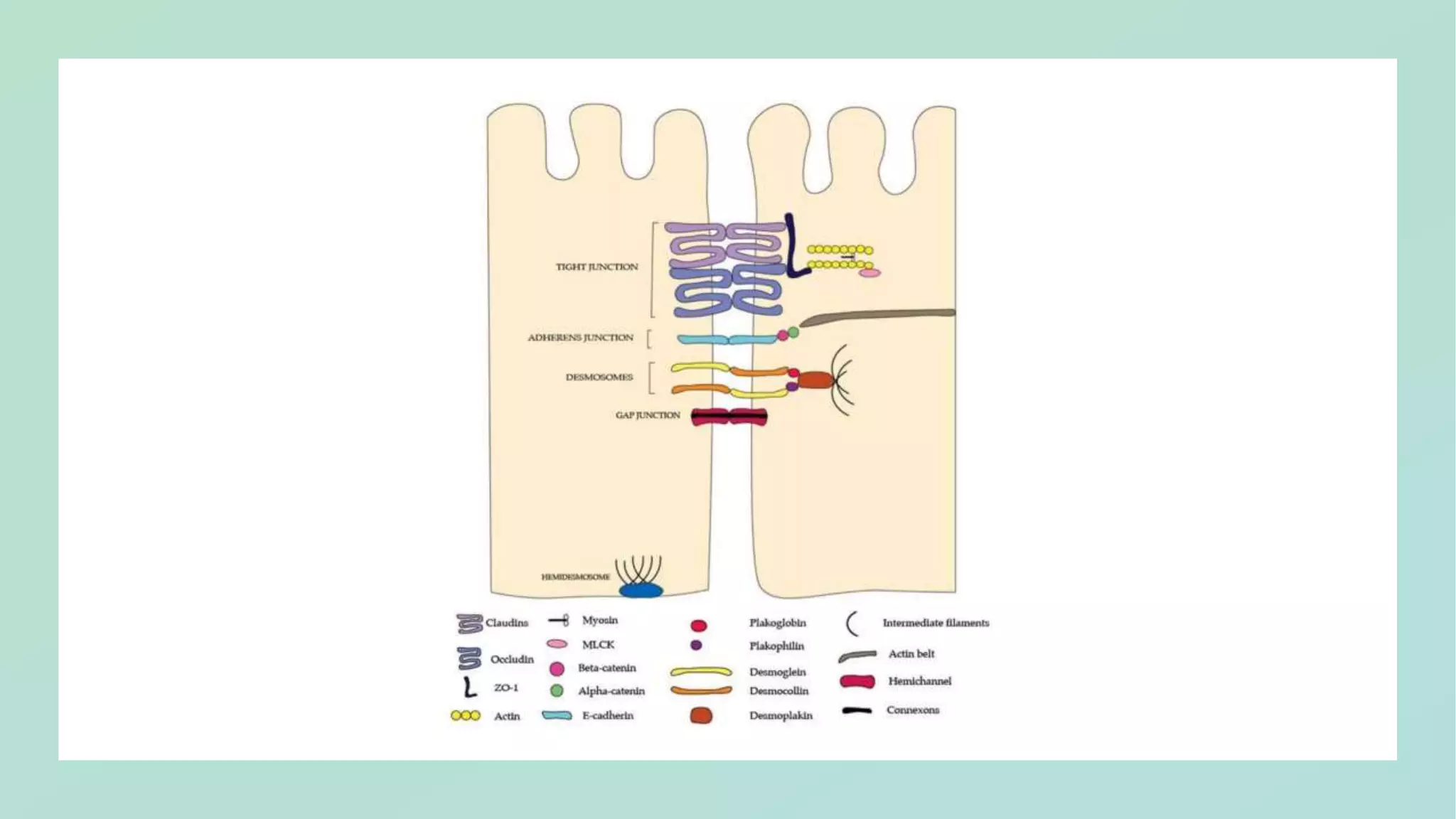


Drug absorption from the gastrointestinal (GI) tract depends on several physiological factors: 1) Gastric emptying and intestinal transit time influence drug absorption by determining how long drugs remain in areas where absorption can occur. Faster emptying and transit generally increase absorption rate. 2) Water fluxes in the GI tract can impact drug dissolution and movement within the lumen, affecting absorption. Considerable water is secreted in the small intestine and mostly reabsorbed. 3) The permeability of drugs is affected by their solubility, ionization state, and lipophilicity, which determine how well drugs can pass through membranes according to the pH partition hypothesis. However, the microclimate pH at the membrane surface can differ
Presentation by Pallerla Naveen Reddy focusing on drug absorption and factors influencing it.
Highlights properties of the GI tract such as permeability, pH partition hypothesis, gastric emptying, intestinal transit time, and other absorption factors.
Discusses the importance of water fluxes due to secretion and reabsorption on drug absorption rates.
Focuses on Fick's first law, influencing factors of drug permeability, and the impact of charge state on drug absorption.
Details the pH partition hypothesis, emphasizing drug ionization, pKa values, and the impact on absorption.Examines the relationship between drug lipophilicity, oil/water partition coefficient, and bioavailability.
Analyzes pH-absorption curves for drug types and highlights deviations from theoretical expectations due to physiological conditions. Explains the concept of the microclimate pH at drug absorption sites and the implications on absorption efficiency.