Downloaded 102 times


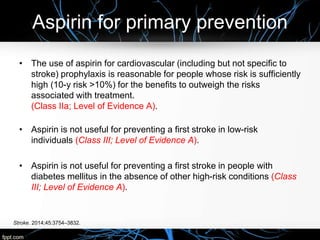
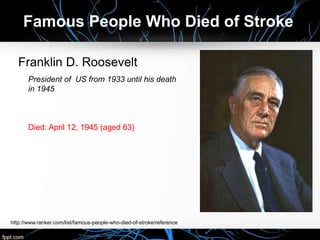
![Phase III AVERROES: stroke or systemic
embolic event
Connolly SJ et al. Presented at ESC 2010; session number 708005-708006.
Available at: http://www.escardio.org/congresses/esc-2010/congress-
reports/Pages/708-3-AVERROES.aspx [Accessed September 2010]
RR = relative risk; CI = confidence interval
Cumulativerisk
0.02
0.04
0.05
0.06
0.07
0
0.01
0.03
0
Months
3 6 9 12 18 21
2791 2720 2541 2124 1541 626 329
2809 2761 2587 2127 1523 617 352
Aspirin
Apixaban
RR 0.46
95% CI: 0.33–0.64
P<0.001
Aspirin
Apixaban](https://image.slidesharecdn.com/primarypreventionofstrokeusamaragab2015-170101165808/85/Primary-prevention-of-stroke-71-320.jpg)
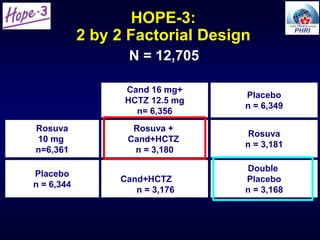
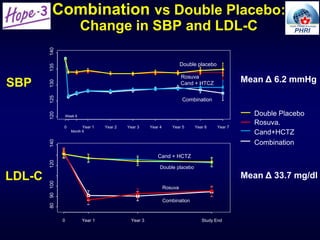
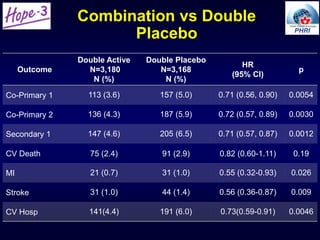
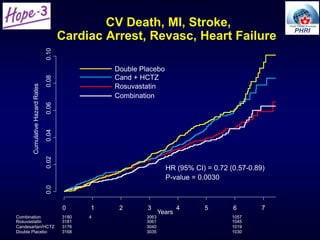
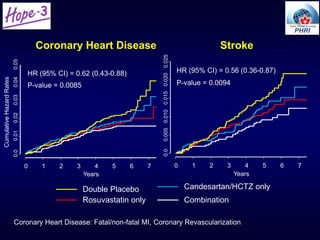
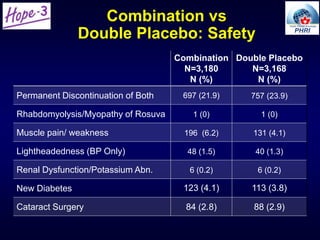


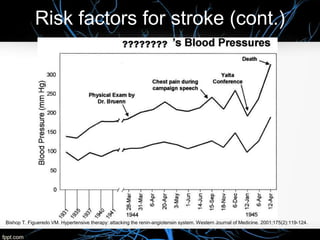


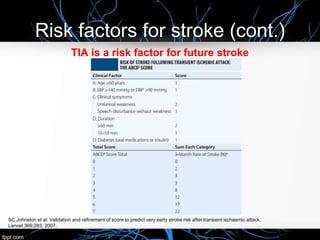
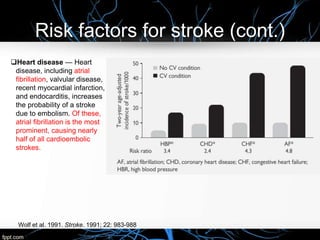
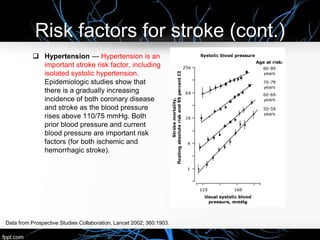
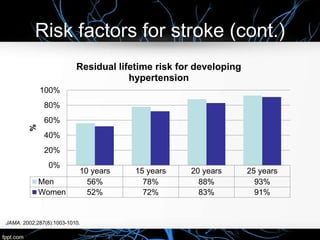
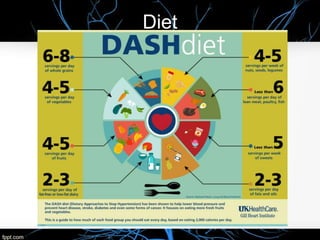
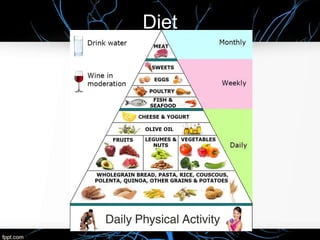
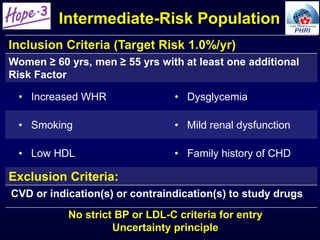
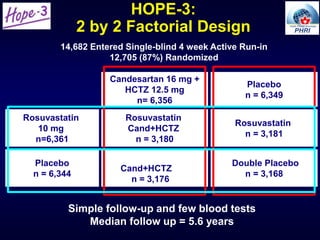
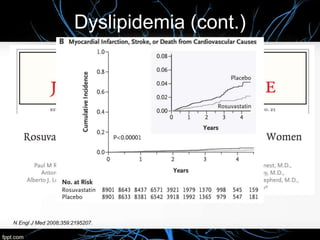
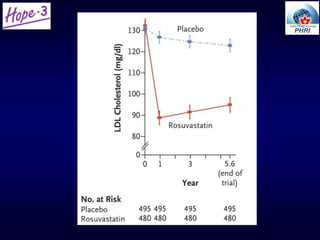
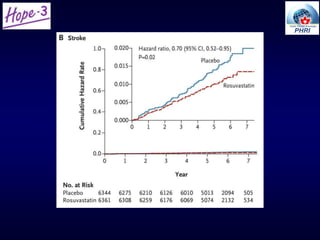
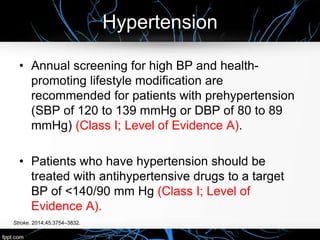
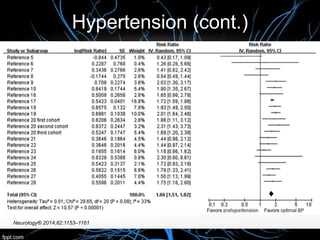
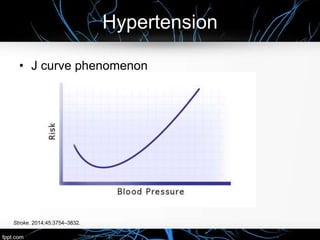
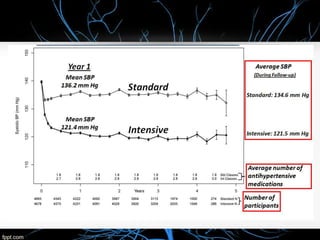
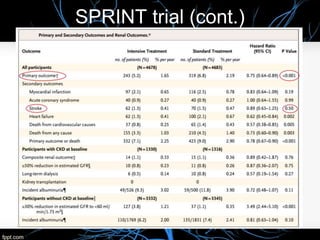
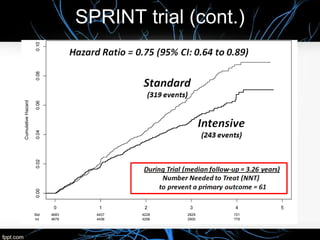
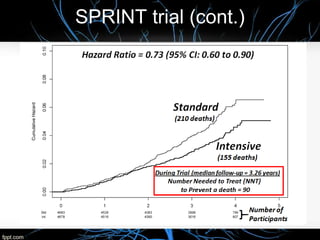
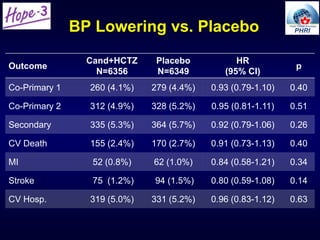
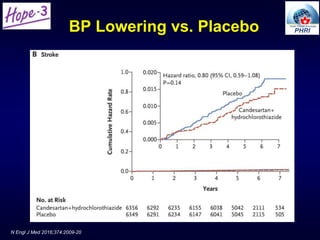
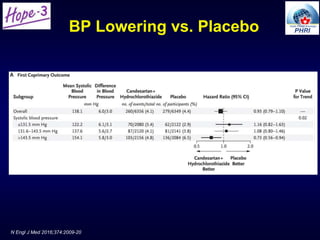
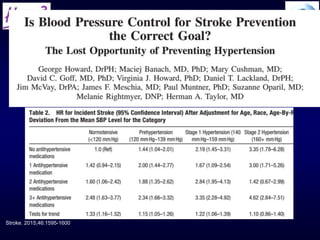
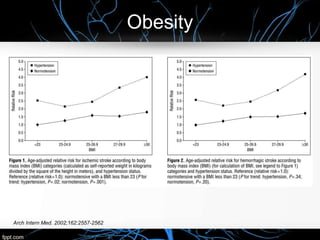
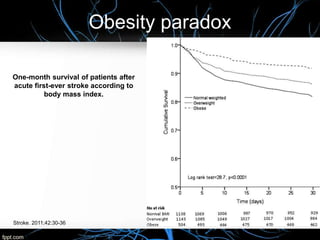
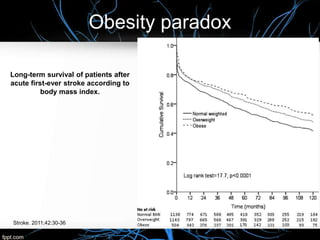
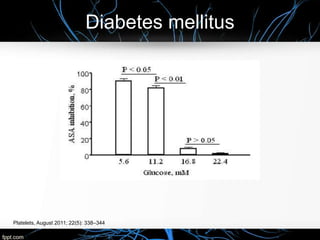
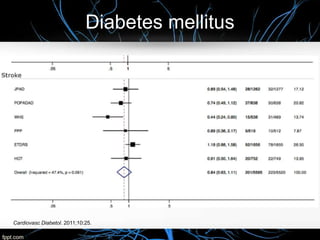
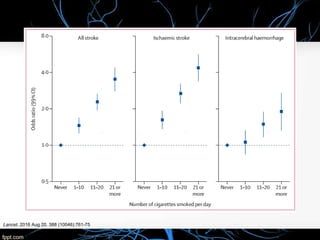
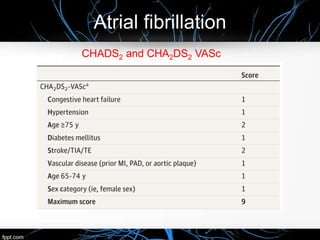
The document discusses the primary prevention of stroke, emphasizing the impact of hypertension, dyslipidemia, and lifestyle factors on stroke risk. It highlights the importance of adhering to the ASA/AHA 2014 guidelines and reviews key trials including SPRINT and HOPE-3 that explore treatment strategies and risk factors. Statistical evidence illustrates that modifying risk factors such as blood pressure, physical activity, and dietary choices can significantly lower the incidence of stroke.











































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)











